
Abstract
Purpose
High acuity units (HAU) are hospital units that provide patients with more acute care and closer monitoring than a general hospital ward but are not as resource intensive as an intensive care unit (ICU). Nevertheless, the impact of opening a HAU on ICU patient outcomes remains poorly defined. We investigated how the creation of a HAU impacted patient outcomes in the ICU.
Methods
This historical cohort study compared ICU patient in-hospital mortality, ICU length of stay (LOS), and hospital LOS before and after the creation of a HAU in a tertiary-care hospital with a medical/surgical ICU between 1 January 2013 and 31 December 2017.
Results
Data from 4,380 patients (984 in the pre-HAU group and 3,396 in the post-HAU group) were analyzed. In this cohort of ICU patients, 360 (37%) died in the pre-HAU group before the creation of a HAU, and 1,074 (32%) died in the post-HAU group after the creation of a HAU. The creation of a HAU was associated with lower relative risk of in-hospital mortality (adjusted risk ratio, 0.80; 95% confidence interval [CI], 0.72 to 0.89; P < 0.001). The creation of a HAU was also associated with reduced ICU and hospital LOS with a 12% increase in the rate of ICU discharge (adjusted sub-distribution hazard ratio [SHR], 1.12; 95% CI, 1.02 to 1.23; P = 0.02) and a 26% increase in the rate of hospital discharge (adjusted SHR, 1.26; 95% CI, 1.14 to 1.39; P < 0.001), when accounting for the competing risk of death.
Conclusions
These data support the hypothesis that the creation of a HAU may be associated with reduced in-hospital mortality, ICU LOS, and hospital LOS for ICU patients.
Résumé
Objectif
Les unités de soins intermédiaires sont des départements hospitaliers qui prodiguent des soins plus aigus et un monitorage plus serré aux patients qu’une unité générale, mais qui ne nécessitent pas autant de ressources qu’une unité de soins intensifs (USI). L’impact de l’ouverture d’une unité de soins intermédiaires sur les devenirs des patients à l’USI n’a pourtant été que peu décrit. Nous avons exploré la façon dont la création d’une unité de soins intermédiaires a eu un impact sur les devenirs des patients à l’USI.
Méthode
Cette étude de cohorte historique a comparé la mortalité hospitalière, la durée de séjour à l’USI et la durée de séjour hospitalier des patients à l’USI avant et après la création d’une unité de soins intermédiaires dans un hôpital de soins tertiaires disposant d’une USI médicale/chirurgicale entre le 1er janvier 2013 et le 31 décembre 2017.
Résultats
Les données de 4380 patients (984 dans le groupe pré unité de soins intermédiaires et 3396 dans le groupe post unité de soins intermédiaires) ont été analysées. Dans cette cohorte de patients de l’USI, 360 (37 %) sont décédés avant la création de l’unité de soins intermédiaires, et 1074 (32 %) sont décédés après. La création d’une unité de soins intermédiaires a été associée à un risque relatif plus faible de mortalité hospitalière (risque relatif ajusté, 0,80; intervalle de confiance [IC] 95 %, 0,72 à 0,89; P < 0,001). La création d’une unité de soins intermédiaires a également été associée à une durée de séjour réduite à l’USI et à l’hôpital, avec une augmentation de 12 % du taux de congé de l’USI (rapport de risque ajusté [RRA], 1,12; IC 95 %, 1,02 à 1,23; P = 0,02) et une augmentation de 26 % du taux de congé de l’hôpital (RRA, 1,26; IC 95 %, 1,14 à 1,39; P < 0,001), en tenant compte du risque concurrent de décès.
Conclusion
Ces données appuient l’hypothèse que la création d’une unité de soins intermédiaires pourrait être associée à une réduction de la mortalité hospitalière, de la durée de séjour à l’USI et de la durée de séjour à l’hôpital pour les patients de l’USI.
Similar content being viewed by others
Critical care beds are increasing in availability in both the United States and Canada.1,2,3 Despite an increasing number of beds in some regions, many critically ill patients still face delays in receiving intensive care unit (ICU)-level care. Delays in transfer of care and/or the mistriage of critically ill patients to the medical ward are associated with worse outcomes for patients.4,5,6,7
High acuity units (HAUs), sometimes called intermediate-level care units, can support ICUs in caring for critically ill patients.8,9,10,11,12,13 High acuity units can provide a higher level of care for patients than the general hospital ward through their higher nurse-to-patient ratios and better access to respiratory therapists and physiotherapists.3 Compared with ICUs, HAUs have lower nurse-to-patient ratios and are generally not able to provide invasive mechanical ventilation or high-dose vasopressor infusions. Overall, HAUs are less resource intensive than ICUs, but more expensive than regular hospital wards.8
Previous literature has shown that HAUs can support ICUs through multiple mechanisms including improving ICU capacity, and functioning as both a “step-up” and “step-down” unit.3,13 These HAUs can admit more stable sub-acutely ill patients, decanting them from the ICU and freeing more ICU beds for patients with higher severity of illness.8,9,10,11,12,13 Additionally, admitting the sickest ward patients who do not meet usual ICU admission criteria to the HAU provides them with a higher level of care that can prevent or reduce the severity of potential progressive clinical deterioration. The HAU can also be a step-down unit for the ICU, providing support for patients who no longer need the ICU but can still benefit from the closer monitoring provided by the HAU. Despite the proposed benefits to patient flow, questions remain about how a HAU affects patient outcomes in mixed medical/surgical ICUs.
We sought to investigate how the creation of a new HAU impacted outcomes for critically ill patients in a large tertiary-care Canadian hospital. Based on the prior literature, we anticipated that opening a HAU would allow critically ill patients to access critical care resources more quickly and to receive staged convalescent care when needed. Therefore, we hypothesized that the creation of the HAU would reduce in-hospital mortality for patients admitted to the ICU. We additionally tested the hypothesis that the creation of a HAU would be associated with decreased ICU and hospital length of stay (LOS).
Methods
We conducted a retrospective before-and-after cohort study and adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations.14 The study protocol was approved by the Fraser Health Research Ethics Board (FHREB) on 8 March 2019. Given that this study was retrospective and deemed low-risk, the FHREB waived the need for consent from patients to participate in this study.
Surrey Memorial Hospital is a 650-bed tertiary-care hospital in Surrey, British Columbia, Canada with a mixed medical/surgical ICU. On 16 June 2014, the hospital opened a new eight-storey critical care tower. This expansion took the ICU from 20 beds to 26 beds and created a 20-bed HAU on the floor above the ICU. It provided the opportunity to investigate how the creation of a HAU impacted outcomes for patients admitted to the ICU.
The HAU was a closed unit staffed with critical care physicians, respiratory therapists, dieticians, physiotherapists, and high acuity-trained nurses with a 1:2 nurse-to-patient ratio. The HAU accepted patients from the emergency department, operating room, other hospital wards, and the ICU. Patients were admitted to the HAU at the discretion of the attending critical care physician if they required non-invasive positive pressure ventilation, vasopressors/inotropes, or either cardiac or other close clinical monitoring for > 24 hr. The attending critical care physician was on-call for both the ICU and the HAU over a 24-hr period, with support from 0–2 medical resident trainees.
We performed a historical cohort study comparing the outcomes for ICU patients before and after the creation of the HAU at Surrey Memorial Hospital. Data were collected from the British Columbia Critical Care database, which is a provincial database that collects patient data from the majority of ICUs in the province. Surrey Memorial Hospital first began inputting data into the database in January 2013 and the last complete year of data entry when this study began was December 2017. We included all adult patients (aged ≥ 16 yr) who were admitted to the ICU from 1 January 2013 to 31 December 2017. We also collected data on the HAU patient population from 16 June 2014 to 31 December 2017.
The exposure was the existence of a HAU in the hospital. Therefore, the control group was the pre-HAU group with patients admitted to the ICU before the HAU was created, from 1 January 2013 until 15 June 2014. The intervention group was the post-HAU group with patients admitted to the ICU after the HAU was created, from 16 June 2014 until 31 December 2017.
The primary outcome was in-hospital mortality. Secondary outcomes were ICU and hospital LOS. The LOS was defined as the day of discharge minus the day of admission.
Baseline demographics collected included age, sex, Acute Physiology And Chronic Health Evaluation (APACHE) II score, admission location, and admission diagnosis. Age was a continuous variable. APACHE II score was a continuous variable and calculated using data from 24 hr after admission to the ICU or HAU. Patients who were discharged from the ICU or HAU within 24 hr, either because of rapid clinical improvement or death, had missing APACHE II scores. Admission location was a categorical variable that included the emergency department, operating room, post-anesthesia recovery unit, general hospital ward (medical or surgical), cardiac care unit, cardiac catheterization lab, external hospital, thoracic surgical care unit, or HAU. Admission diagnosis was a categorical variable that included sepsis, cardiac, toxin, renal failure, airway obstruction, neurologic, asthma, gastrointestinal bleed, chronic obstructive pulmonary disease, and others. These categories were created using the nine most common admission diagnoses and the “others” category for the remainder. Do not resuscitate (DNR) status was collected; DNR status was a dichotomous variable defined as true if a patient or their substitute decision-maker decided not to accept cardiopulmonary resuscitation during their stay in either the ICU or HAU.
Statistical analysis
The unit of analysis was ICU admission. All patients admitted to the ICU during the study period were included in the analysis, therefore a sample size calculation was not performed. All analyses were done as complete case analyses. The baseline covariates for the pre-HAU group and the post-HAU group were summarized using descriptive statistics and compared. Continuous variables were presented as mean (standard deviation) or median [interquartile range] and compared using Student’s t tests. Dichotomous or categorical variables were presented as total number (%) and analyzed using Chi square tests. We used both unadjusted and adjusted generalized linear models with log link functions to test the association between the presence of a HAU and in-hospital mortality. The adjusted model controlled for the baseline covariates. Since this complete case-adjusted model excluded all patients who were transferred out of the ICU or who died within 24 hr of admission to the ICU because they would not have APACHE II scores, a sensitivity analysis was performed using the same complete case-adjusted model without controlling for APACHE II score.
Other authors have described that in-hospital mortality among ICU patients has declined over time.15 This reduction in mortality may be attributable to better systems of care and multiple small improvements in the administration of care to critically ill patients resulting in an observable difference over time. Our primary model assumed that this trend in reduction of mortality over time was not strong enough to confound the association between mortality and the presence of a HAU in this before-and-after study over five years. To test this assumption, we performed a sensitivity analysis including year as a nominal variable in the adjusted model.
The secondary outcomes, ICU LOS and hospital LOS, were analyzed using adjusted cumulative incidence competing risks models producing sub-distribution hazard ratios (SHR) because in-hospital mortality was a significant source of informative censoring that would confound the relationship between LOS and the presence of the HAU.16,17 These adjusted models controlled for the baseline covariates. We performed all analyses using Stata (IC version 14.2 for Windows; StataCorp LLC, College Station, TX, USA). A P value of < 0.05 was considered statistically significant and analyses were not adjusted for multiple comparisons.
Results
During the study period, 4,380 patients were admitted to the ICU at Surrey Memorial Hospital. Nine hundred and eighty-four patients were admitted before the creation of the HAU and 3,396 patients were admitted after the creation of the HAU.
Table 1 shows the baseline demographics and patient outcomes for the pre-HAU and post-HAU groups, as well as patients admitted to the HAU during the post-HAU study period. The baseline demographics were well balanced. Age, APACHE II score, and admission diagnosis were similar between the pre-HAU and post-HAU groups, while sex and admission location differed. The post-HAU group consisted of more male patients and had fewer patients admitted to the ICU from the ward, more transfers from other facilities, and more admissions from the HAU. A DNR status occurred in 32% of pre-HAU patients, 36% of post-HAU patients, and 30% of HAU patients. During the post-HAU study period, 13% of patients who were admitted to the ICU were transferred from the HAU and 13% of patients who were discharged from ICU were transferred to the HAU.
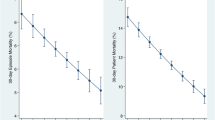
The results of our study can be seen in Table 2 and model details can be seen in eTable 1 and eTable 2 (available as Electronic Supplementary Material). In-hospital mortality occurred in 1,074 of 3,396 patients (32%) in the post-HAU group and 360 of 984 patients (37%) in the pre-HAU group. Intensive care unit patients had 14% lower risk of death after the creation of the HAU (unadjusted risk ratio [RR], 0.86; 95% CI, 0.79 to 0.95; P = 0.003). After adjusting for patient age, sex, APACHE II score, admission location, and admission diagnosis, critically ill patients had 20% lower risk of death after the creation of the HAU (adjusted RR, 0.80; 95% CI, 0.72 to 0.89; P < 0.001). Figure 1 shows the adjusted predicted mortality over time. In June 2014, with the creation of the HAU, there was a reduction in mortality, although the creation of the HAU did not alter the overall downward trend in mortality that previously existed.

Predicted mortality based on the adjusted model controlling for age, sex, APACHE II score, admission location, and admission diagnosis. APACHE = Acute Physiology And Chronic Health Evaluation
In our first sensitivity analysis, we examined the influence of missing APACHE II data. The study cohort had 588 patients with missing APACHE II data—446 (13%) in the post-HAU group and 142 (14%) in the pre-HAU group. The adjusted model controlling for age, sex, admission location, and admission diagnosis but not APACHE II score also found a similar significant association between mortality and the creation of a HAU with a RR of 0.87 (95% CI, 0.79 to 0.96; P = 0.004). In our second sensitivity analysis including year as a covariate, the adjusted model found a significant association between mortality and the creation of the HAU with a RR of 0.76 (95% CI, 0.62 to 0.94; P = 0.01).
Cumulative incidence competing risks regression found the creation of a HAU was associated with a 12% increase in the rate of ICU discharge (adjusted SHR, 1.12; 95% CI, 1.02 to 1.23; P = 0.02) (Fig. 2) and with a 26% increase in the rate of hospital discharge (adjusted SHR, 1.26; 95% CI, 1.14 to 1.39; P < 0.001). The associated cumulative incidence curves can be seen in Figs 2 and 3, respectively.

Cumulative incidence of discharge from intensive care unit

Cumulative incidence of discharge from hospital
Discussion
We found that the creation of a HAU was associated with reduced in-hospital mortality for ICU patients. We also found that the presence of a HAU was associated with a reduction in ICU and hospital LOS.
Previous studies showed that a small HAU can improve throughput and reduce patient LOS without increasing mortality in specialized ICUs.10,12,13 We found that a larger HAU may reduce patient mortality in a large, mixed medical/surgical ICU. The demographic data show that this benefit may have been derived in part by using the HAU as a step-up unit because in the post-HAU period 13% of patients who were admitted to the ICU were transferred from the HAU. The HAU’s function as a step-down unit may also have contributed as 13% of ICU patients were discharged to the HAU. Unfortunately, because of missing data we were unable to analyze the difference in time between admission and arrival to the ICU to determine if the HAU improving ICU capacity facilitated more rapid admission into the ICU. The association between reduction in mortality and the creation of the HAU persisted in our sensitivity analysis suggesting the results are independent of a trend in reduction in ICU patient mortality over time.
The HAU functioning as a step-down unit may also have impacted ICU and hospital LOS. The actual ICU LOS was similar in the pre-HAU and post-HAU groups, while the actual hospital LOS reduced by almost two days. Nevertheless, these metrics do not account for confounders, nor do they account for the competing risk of death that occurred in over 30% of patients in both groups. The adjusted competing risk regression analysis estimated a 12% and 26% improvement in the rate of ICU and hospital discharge, respectively. Intensive care unit discharge may have been facilitated by the HAU being a step-down unit for frailer patients who were not ready for discharge from the ICU to the hospital ward. Earlier hospital discharge may have been due to the HAU being a step-down unit that is able to provide more intensive physiotherapy and closer nursing care than the hospital ward, resulting in a faster overall recovery for the sickest patients in the hospital.
Our study has several limitations. First, our study was a retrospective, before-and-after design and as such, despite conducting both adjusted analyses and sensitivity analyses, the results remain susceptible to residual confounding. Second, our study was conducted at a single, tertiary-care centre with a medical/surgical ICU and the generalizability of these results can only be verified through replication. Results may also be different in ICUs that contain cardiac surgery, neurosurgery, or trauma patients. Third, we were not able to adjust for coincidental staffing and administrative changes that occurred in temporal association with the creation of the HAU, which may have also confounded the relationship between the exposure and primary outcome. Fourth, at the same time the HAU was created, the ICU expanded from 20 beds to 26 beds. Higher ICU occupancy has previously been shown to be associated with increased inpatient mortality,18 so increasing ICU beds may have reduced ICU occupancy contributing to our observed reduction in mortality. Unfortunately, ICU occupancy data were not available for analysis. Nevertheless, we do not believe the additional beds had a significant impact on patient outcomes as the ICU was staffed for 21 beds and very rarely admitted additional patients to go over capacity. And lastly, the study design is susceptible to selection bias through differential entry into the study during the pre-HAU and post-HAU periods. If sicker patients or critically ill patients with limitations to their goals of care were preferentially admitted into the HAU instead of the ICU during the post-HAU period, the results would be biased toward showing an association between reduced ICU mortality and the creation of a HAU. Nevertheless, we believe this bias is unlikely to have occurred since the HAU patients had similar proportions of DNR status and had lower APACHE II scores and mortality than the ICU patients. This is probably because the HAU could not admit sicker patients who were mechanically ventilated, on high-dose vasopressors, or requiring continuous renal replacement therapy.
Our findings add to the growing literature supporting HAUs as potentially important units in tertiary-care hospitals. High acuity units have previously been shown to provide safe and cost-effective care for their patients, but we have shown that opening a HAU may facilitate better outcomes for ICU patients.8,19,20 Our findings also suggest that opening a HAU may reduce ICU and hospital LOS for ICU patients. Given both demonstrated and predicted increase in demand for critical care beds in Canada, our results support the trend of increasing expansion of HAU beds.2
Conclusion
We found that the addition of a HAU to a hospital was associated with reduced in-hospital mortality, ICU LOS, and hospital LOS for patients admitted to the ICU. Further studies are needed to determine if this is a causal relationship and if these results are generalizable to all hospital settings.
References
Wallace DJ, Angus DC, Seymour CW, Barnato AE, Kahn JM. Critical care bed growth in the United States: a comparison of regional and national trends. Am J Respir Crit Care Med 2015; 191: 410-6.
Canadian Institute for Health Information. Care in Canadian ICUs. August 2016. Available from URL: https://secure.cihi.ca/free_products/ICU_Report_EN.pdf (accessed May 2020).
Prin M, Wunsch H. The role of stepdown beds in hospital care. Am J Respir Crit Care Med 2014; 190: 1210-6.
Cardoso LT, Grion CM, Matsuo T, et al. Impact of delayed admission to intensive care units on mortality of critically ill patients: a cohort study. Crit Care 2011; DOI: https://doi.org/10.1186/cc9975.
Fowler RA, Abdelmalik P, Wood G, et al. Critical care capacity in Canada: results of a national cross-sectional study. Crit Care 2015; Doi: https://doi.org/10.1186/s13054-015-0852-6.
Liu V, Kipnis P, Rizk NW, Escobar GJ. Adverse outcomes associated with delayed intensive care unit transfers in an integrated healthcare system. J Hosp Med 2012; 7: 224-30.
Churpek MM, Wendlandt B, Zadravecz FJ, Adhikari R, Winslow C, Edelson DP. Association between intensive care unit transfer delay and hospital mortality: a multicenter investigation. J Hosp Med 2016; 11: 757-62.
Lamb LC, DiFiori MM, Calafell J, Comey CH, Shapiro DS, Feeney JM. Is a stepdown unit safe for patients with mild traumatic intracranial hemorrhages? Eur J Trauma Emerg Surg 2018; 44: 897-901.
Lawlor DK, Lovell MB, DeRose G, Forbes TL, Harris KA. Is intensive care necessary after elective abdominal aortic aneurysm repair? Can J Surg 2004; 47: 359-63.
Solberg BC, Dirksen CD, Nieman FH, et al. Introducing an integrated intermediate care unit improves ICU utilization: a prospective intervention study. BMC Anesthesiol 2014; DOI: https://doi.org/10.1186/1471-2253-14-76.
Fiebach NH, Cook EF, Lee TH, et al. Outcomes in patients with myocardial infarction who are initially admitted to stepdown units: data from the Multicenter Chest Pain Study. Am J Med 1990; 89: 15-20.
Eachempati SR, Hydo LJ, Barie PS. The effect of an intermediate care unit on the demographics and outcomes of a surgical intensive care unit population. Arch Surg 2004; 139: 315-9.
Gershengorn HB, Chan CW, Xu Y, et al. The impact of opening a medical step-down unit on medically critically ill patient outcomes and throughput: a difference-in-differences analysis. J Intensive Care Med 2020; 35: 425-37.
Von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Bull World Health Organ 2007; 85: 867-72.
Zimmerman JE, Kramer AA, Knaus WA. Changes in hospital mortality for United States intensive care unit admissions from 1988 to 2012. Crit Care 2013; DOI: https://doi.org/10.1186/cc12695.
Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc 1999; 94: 496-509.
Harhay MO, Ratcliffe SJ, Small DS, Suttner LH, Crowther MJ, Halpern SD. Measuring and analyzing length of stay in critical care trials. Med Care 2019; 57: e53-9.
Fergusson NA, Ahkioon S, Nagarajan M, et al. Association of intensive care unit occupancy during admission and inpatient mortality: a retrospective cohort study. Can J Anesth 2020; 67: 213-24.
Chou YS, Lin HY, Weng YM, et al. Step-down units are cost-effective alternatives to coronary care units with non-inferior outcomes in the management of ST-elevation myocardial infarction patients after successful primary percutaneous coronary intervention. Intern Emerg Med 2020; 15: 59-66.
Richards BF, Fleming JB, Shannon CN, Walters BC, Harrigan MR. Safety and cost effectiveness of step-down unit admission following elective neurointerventional procedures. J Neurointerv Surg 2012; 4: 390-2.
Author contributions
Anish R. Mitra and Jennifer P. Stevens designed, analyzed, and interpreted the study data. Donald E. G. Griesdale and Gregory Haljan contributed to study design. Ashley O’Donoghue contributed to data analysis. All authors were major contributors in writing the manuscript.
Disclosures
None.
Financial statement
Jennifer P. Stevens is supported by grant number K08HS024288 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not represent the official views of the Agency for Healthcare Research and Quality. Jennifer P. Stevens is also supported by the Doris Duke Charitable Foundation. Donald E. G. Griesdale received funding through a Health-Professional Investigator Award from the Michael Smith Foundation for Health Research.
Editorial responsibility
This submission was handled by Dr. Hilary P. Grocott, Editor-in-Chief, Canadian Journal of Anesthesia.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mitra, A.R., Griesdale, D.E.G., Haljan, G. et al. How the high acuity unit changes mortality in the intensive care unit: a retrospective before-and-after study. Can J Anesth/J Can Anesth 67, 1507–1514 (2020). https://doi.org/10.1007/s12630-020-01775-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-020-01775-5