




- COVID-19
- Biosimilars
- Cataract Therapeutics
- DME
- Gene Therapy
- Workplace
- Ptosis
- Optic Relief
- Imaging
- Geographic Atrophy
- AMD
- Presbyopia
- Ocular Surface Disease
- Practice Management
- Pediatrics
- Surgery
- Therapeutics
- Optometry
- Retina
- Cataract
- Pharmacy
- IOL
- Dry Eye
- Understanding Antibiotic Resistance
- Refractive
- Cornea
- Glaucoma
- OCT
- Ocular Allergy
- Clinical Diagnosis
- Technology
Ultra-widefield imaging can enhance efficiency for practices
Physicians can discover, diagnose, document, treat diseases that might go undetected



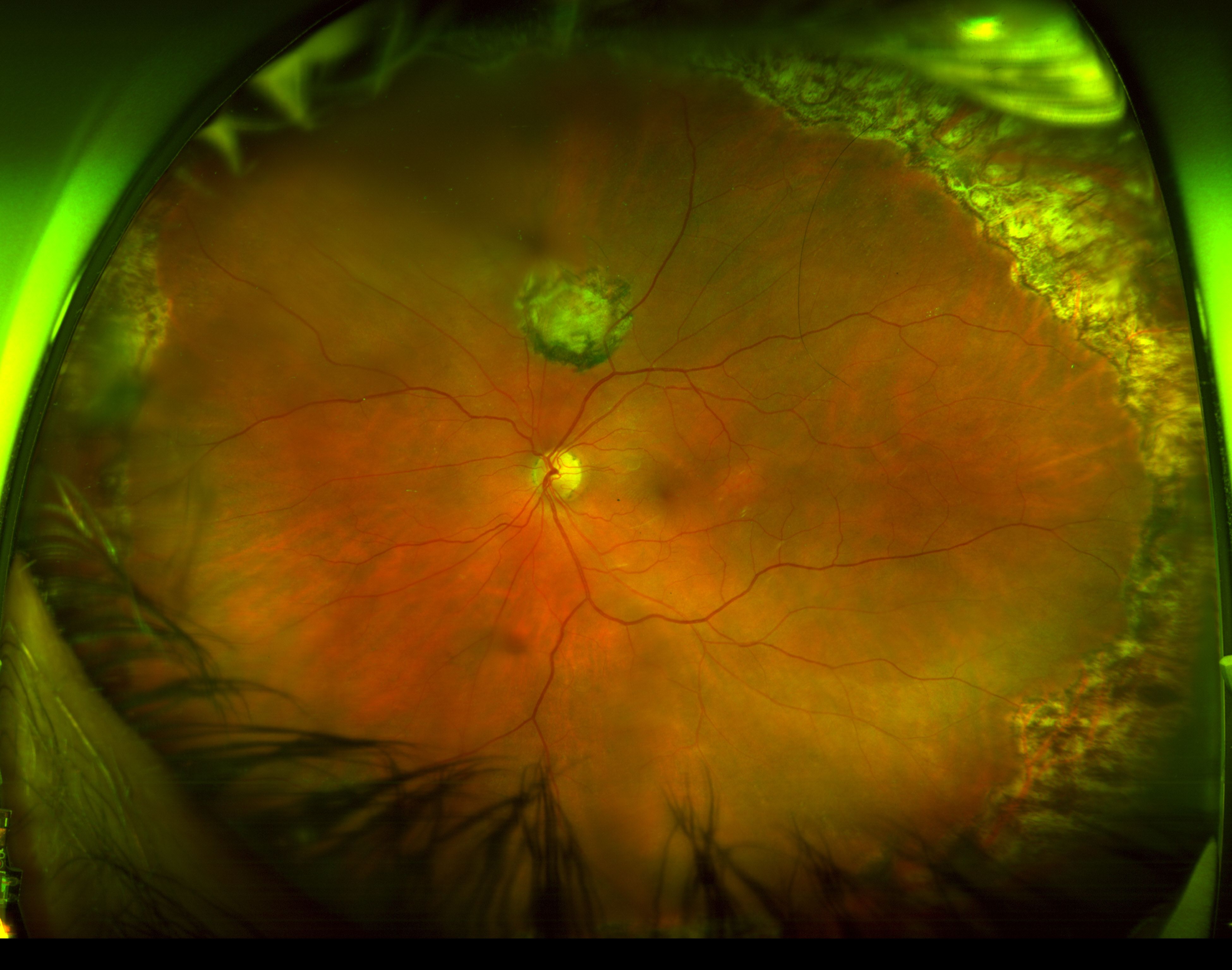
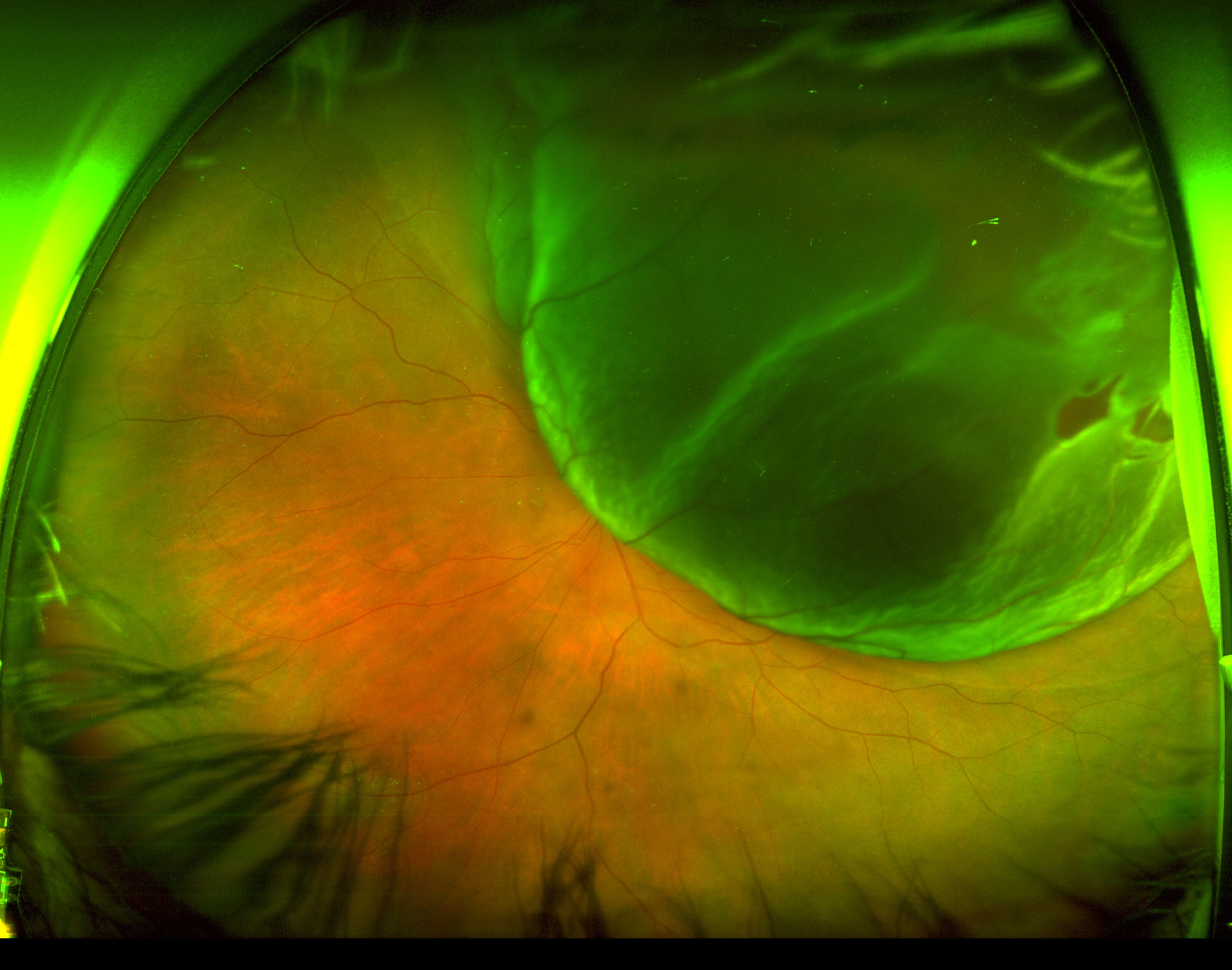
 and L2 (lower right) show how OS before and after retinal detachment repair. These photos are helpful in patient education in addition to documentation.")
L1 (above) and L2 (lower right) show OS before and after retinal detachment repair. These photos are helpful in patient education in addition to documentation.

Special to Ophthalmology Times®
Like most physicians, I am always interested in technology that can elevate patient care.
However, as a solo practitioner in a competitive market, I must be sure that any new technology I consider will have a reasonable financial return.
The optomap ultra-widefield (UWF) imaging devices (Optos) are an example of technology that can simultaneously improve patient care and help grow the practice.
UWF retinal imaging, as defined by the International Wide Field Study Group, refers to a single-capture image encompassing retinal anatomy anterior to the vortex vein ampullae in all 4 quadrants.1
Studies show that UWF imaging helps doctors discover, diagnose, document, and treat pathology that might go undetected using traditional exams and equipment.2-4 These clinical advantages can save vision.
Related: Ultra-widefield imaging adding depth to pediatric ophthalmology
A less-obvious benefit to UWF imaging is that these clinical applications equate to quantifiable practice efficiencies.
Since adding UWF imaging to the practice, we have enjoyed faster patient throughput, as well as increases in referrals and patient satisfaction, resulting in significant practice growth.
Before acquiring our Optos UWF imaging device, we used a digital fundus camera, which meant investing significant time and effort to obtain quality images.
The UWF device images more than 80% of the retina in a single capture in less than half a second, and it is always in focus.

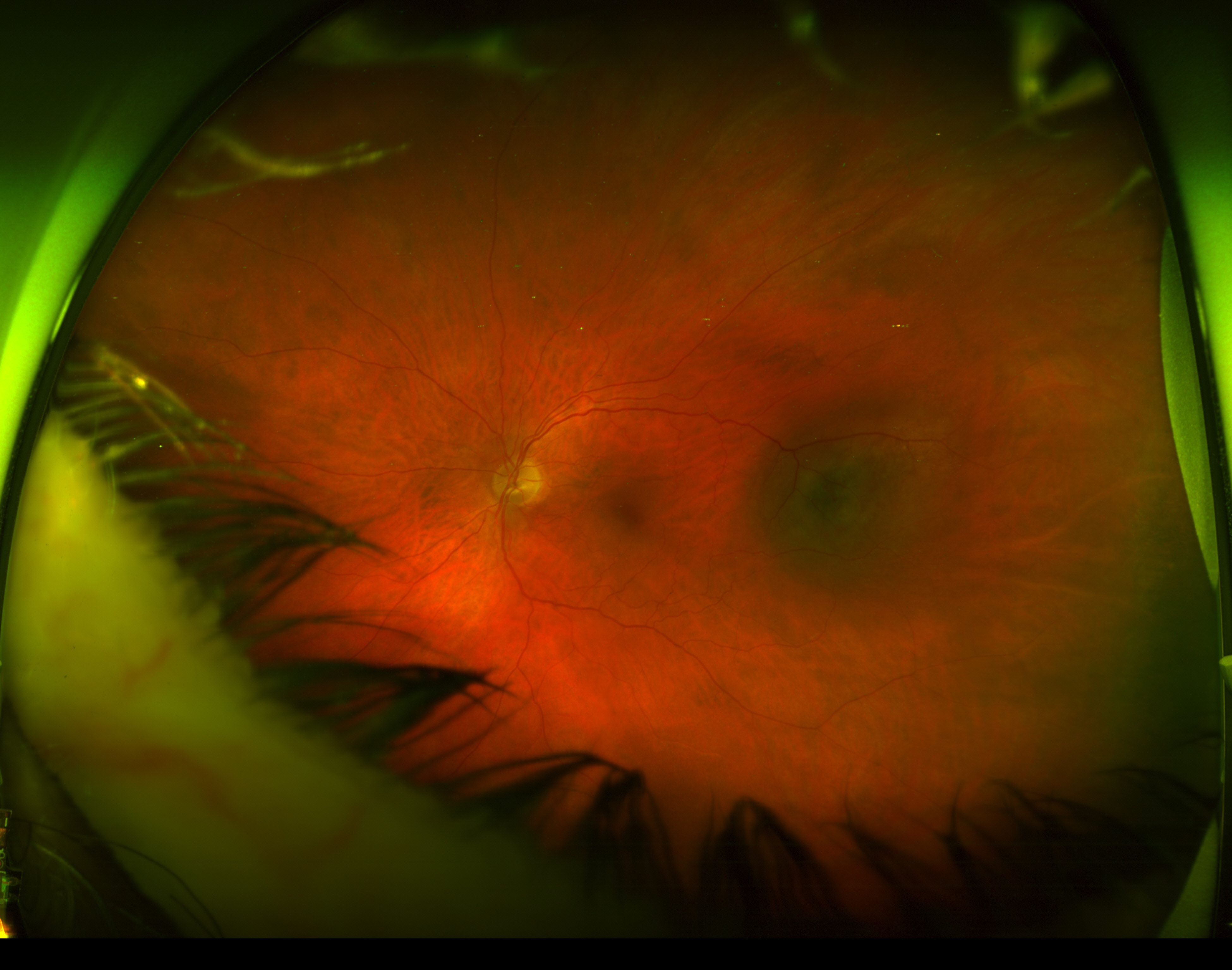
L3-S OS choroidal melanoma diagnosed as "pigmentary changes" by another ophthalmologist a few weeks before visit. Again the widefield photo allows the physician to appreciate the elevation of the lesion.
These UWF imaging devices use cSLO technology, which means they can image effectively through an undilated pupil (and even through most cataracts), contributing significantly to practice efficiency.
By reducing the waiting and patient flow issues incurred during the dilation process, we are able to get patients in and out of the office much more quickly.
The UWF imaging device also enhances efficiency by enabling me to delegate the imaging function to our technicians. All staff members are trained to operate the device.
The learning curve is short and is much easier to use than our previous fundus camera, so staff quickly became adept at capturing and previewing the images.
Related: Coming to terms with 'ultra-widefield' and 'widefield' imaging
As a result of their involvement, staff members often recognize situations when I might require further testing.
When a patient presents with new- onset floaters, I walk into the exam room already knowing where the tear is located because my technician has already captured an optomap image.
Our patients appreciate the benefits this technology offers. Those who are 20/20 uncorrected postoperatively are delighted to be imaged and out the door quickly rather than being dilated and dealing with the associated discomfort and blurred vision for hours afterward.
Of course, dilated fundus exams are still the standard of care. We dilate virtually every patient on their first visit, but if things are stable on follow-up, we may utilize the UWF device to visualize the posterior segment.
For patients who refuse to be dilated, a UWF image that shows no pathology helps me feel more comfortable letting the patient go without dilation.
When the UWF shows peripheral pathology, such as a choroidal mass or a possible tear, I show the optomap image to help the patient understand the need.
Related: UWF imaging contributes to earlier disease detection


Benefits to the bottom line
Although patient care is always our top priority, a healthy bottom line is key to growth and longevity, and we have realized several financial benefits by adopting UWF.
First, it enables us to see more patients. In addition, because peripheral imaging allows us to detect more pathology, we submit more image claims for reimbursement.
We are billing approximately 5 additional images per day because of the increased patient volume, field of view, anddetail achieved with this technology.
A final benefit is that we have increased patient volume specifically via word-of-mouth referrals from patients who appreciate the UWF exam.
The UWF device has design features that contribute to better patient interactions, better care, and practice efficiency.
For example, the ability to compare images taken at various points in time either side by side or with the overlaying feature is invaluable. Sometimes, I will see a nevus and wonder, “I did not comment on this last year, is it something new that I should be more concerned about?”
To be able to look back and confirm the status of pathology at the previous visit is helpful.
Historical images saved in patients’ files are an important medicolegal backup. In many cases, the crux of a lawsuit is whether the physician missed something (a tear, tumor etc).
Related: Ultra-widefield OCT 'may be the only imaging needed' to manage PDR
Summary
Relying on our UWF imaging device enables me to finish my busy clinic work on time—which is appreciated by my family, my staff, and my patients. Dilating only the patients who require it and locating pathology rapidly allows me to operate more efficiently and provide better patient care.
UWF is fast becoming standard-of-care testing in comprehensive ophthalmology. Research in the management of diabetic retinopathy has shown that peripheral lesions identified with UWF imaging are associated with increased risk of disease progression, and identifying these lesions often affects diabetic retinopathy severity grading.2
This should convince ophthalmologists to consider adding UWF to their practice.
About the author
David A. Goldman, MD
e: david@goldmaneye.com
Dr. Goldman is founder and CEO of GoldmanEye, Palm Beach Gardens. He is a speaker and consultant for Optos.
---
References
1. Choudhry N. Classification & guidelines for wide field imaging: recommendations from the International Wide Field Imaging Study Group. Poster session presented at: 51st Annual Retina Society Meeting; 2018 Sept 12-15; San Francisco, CA.
2. Silva PS, Cavallerano JD, Haddad NMN, et al. Peripheral lesions identified on ultrawide field imaging predict increased risk of diabetic retinopathy progression over 4 years. Ophthalmology. 2015;122(5):949-956.
3. Campbell JP, Leder HA, Sepah YJ, et al.Wide-field retinal imaging in the management of noninfectious posterior uveitis. Am J Ophthalmol. 2012;154(5)908-911.
4. Aiello LP, Odia I, Glassman AR, et al. Comparison of early treatment diabetic retinopathy study standard 7-field imaging with ultrawide-field imaging for determining severity of diabetic retinopathy [pahead of print ]. JAMA Ophthalmol.doi:10.1001/jamaophthalmol.2018.4982



























