




- COVID-19
- Biosimilars
- Cataract Therapeutics
- DME
- Gene Therapy
- Workplace
- Ptosis
- Optic Relief
- Imaging
- Geographic Atrophy
- AMD
- Presbyopia
- Ocular Surface Disease
- Practice Management
- Pediatrics
- Surgery
- Therapeutics
- Optometry
- Retina
- Cataract
- Pharmacy
- IOL
- Dry Eye
- Understanding Antibiotic Resistance
- Refractive
- Cornea
- Glaucoma
- OCT
- Ocular Allergy
- Clinical Diagnosis
- Technology
Study targets results of MIGS device versus trabeculectomy


This article was reviewed by N. Douglas Baker, MD
A new study is one of the first head-to-head clinical reviews comparing a minimally invasive glaucoma surgery (MIGS) device with trabeculectomy in patients with primary open-angle glaucoma (POAG).
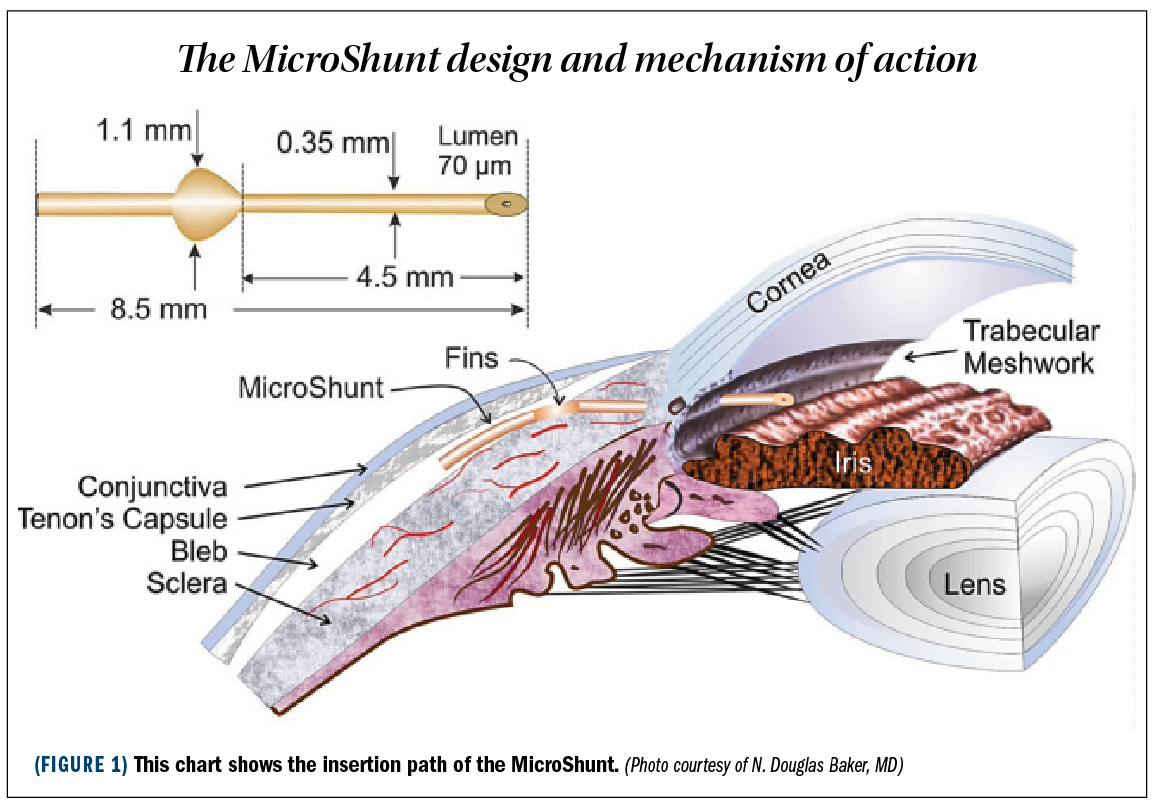
The MicroShunt (Santen) is a subconjunctival glaucoma device made from polystyrene-block-isobutylene-block-styrene (SIBS) material. It is 8.5 mm in length, has a 70-μm lumen, and is highly biocompatible. It enters the anterior chamber at the trabecular meshwork level and forms an aqueous lake beneath the conjunctiva and Tenon’s capsule 3 mm to 6 mm posterior to the limbus.
Related:
Douglas Baker, MD, and colleagues have presented 1-year results from a 2-year study to assess the safety and effectiveness of stand-alone MicroShunt surgery (Figure 1) versus trabeculectomy in patients with POAG.
The randomized, single-masked study was conducted at 29 sites, 24 of which were in the United States.
Patients were between the ages of 40 and 85 years with POAG and were on the maximum tolerated amount of glaucoma medications.
The exclusion criteria were previous conjunctival incisional surgery, aphakia, angle closure, and secondary open-angle glaucomas such as post trauma, pseudoexfoliation, or pigment dispersion.
Related: Minimally invasive glaucoma shunt delivers for patients
Key effectiveness end points
The primary outcome the investigators were looking for was a reduction in IOP of 20% or greater at 1 year, without increasing the number of medications from baseline.
They measured IOP over time, number of glaucoma medications, adverse events (AEs), incidence of persistent hypotony, postoperative interventions, and corneal endothelial cell density.
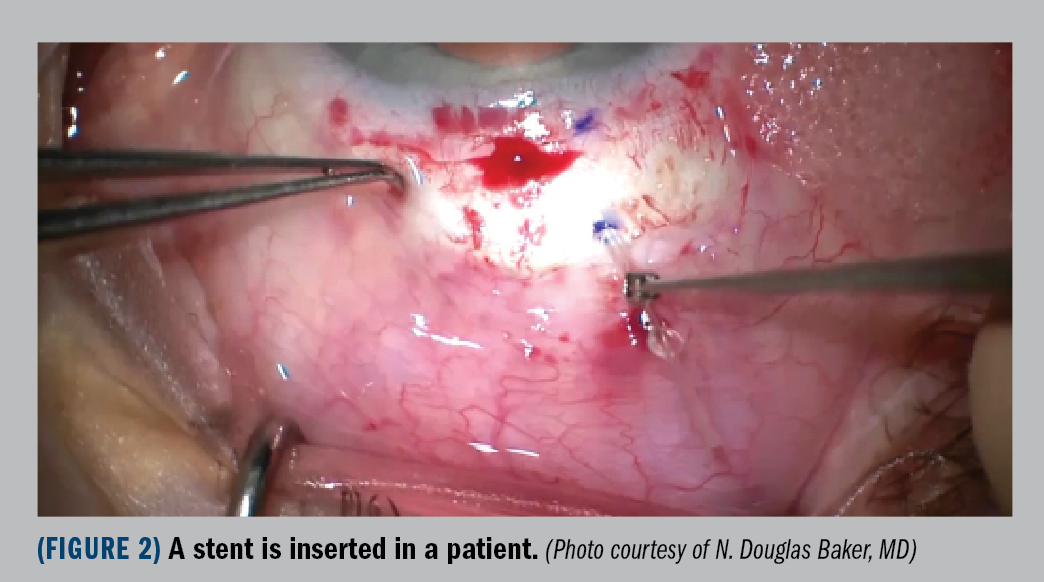
For the procedure (Figure 2), the conjunctiva and Tenon’s capsule were removed at the limbus as a unit. The mytomycin (0.2 mg/mL)–soaked Weck-Cel sponge was placed on the sclera and beneath the Tenon’s for 2 minutes. The initial incision in the sclera is 3 mm posterior to the limbus, and the blade enters the anterior chamber at the trabecular meshwork level.


Within the overall study population, the primary effectiveness end point was met 53.9% of the time with the MicroShunt and 72.7% of the time with trabeculectomy.
If the focus is placed on the group with IOP 21 mm Hg or greater, the MicroShunt met the primary end point 63.8% of the time and trabeculectomy 75% of the time.
Looking at the mean IOP over time, starting at baseline at 21.1 mm Hg, at 1 year the mean in patients with the MicroShunt was 14.2 mm Hg and with the trabeculectomy, 11.2 mm Hg. The mean number of glaucoma medications was 3 at baseline, and after intervention at the end of 1 year, 0.6 medications for the MicroShunt and 0.3 for the trabeculectomy.
Related: Glaucoma treatment alternatives: Thinking outside the box
Adverse events
There was a 5.2% loss in corneal cell density with the MicroShunt, and a 6.9% loss with trabeculectomy. Persistent ocular hypotony occurred 3.0% of the time with the MicroShunt and 9.9% with trabeculectomy. Cataract progression was seen 12.2% of the time in the MicroShunt group and 17.6% in the trabeculectomy group.
For visual acuity, loss of more than 2 lines of best-corrected visual acuity occurred 11.1% of the time in patients with the MicroShunt and 14.5% in those who had trabeculectomy. Choroidal effusion occurred in 4.8% of those with the MicroShunt and in 7.6% with trabeculectomy.
Postoperative interventions included suture lysis and medication change, occurring in 40.8% of patients with the MicroShunt and in 67.4% of those who received trabeculectomy. There were no reports of endophthalmitis in either group at 1 year.
Related: Microinvasive glaucoma surgery in children: Is there a role?
Conclusions
This was a prospective randomized study conducted in patients with primary open-angle glaucoma taking the maximum-tolerated number of glaucoma medications.
Both trabeculectomy and MicroShunt implantation resulted in a reduction in IOP and supplemental glaucoma medications at 1 year.
In the MicroShunt group, 53.9% of patients experienced a 20% or greater decrease in mean diurnal intra-operative pressure from baseline to year 1.
This increased to 63.8% in the group that had IOP 21 mm Hg or greater when they entered the study. There was a reduction in mean diurnal IOP, from 21.1 mm Hg at baseline to 14.2 at 1 year.
The mean number of medications decreased from 3.1 to 0.6 at 1 year and 71.6% of patients were medication free at 1 year. Incidents of AEs and corneal endothelial cell loss were similar between the 2 groups, and there were no reports of endophthalmitis at 1 year.
Related: Genetic variants linked with onset, progression of POAG
Practical applications
The study provides 1-year data on the MicroShunt from 29 sites in the United States, the Netherlands, Spain, Italy, France, and the United Kingdom. Patients with POAG on maximum-tolerated medical therapy (baseline IOP, 15-40 mm Hg) and no previous history of conjunctival surgery were included.
In the study, patients with uncontrolled POAG who underwent MicroShunt implantation achieved, on average, IOP of less than 15 mm Hg up to 1 year after surgery.
Read more by Steve Lenier
---
N. Douglas Baker, MD
e:bakerdoug217@gmail.com
N. Douglas Baker, MD, is a consultant to Santen.



























