Prakash Lab COVID-19 Response Group Working Draft Document
Document #002, rev. 2020-05-10 draft Not an approved medical device
Pneumask: Reusable Full-Face Snorkel Mask PPE Project
Repurposing full-face snorkel masks with a 3D printed N95 filter attachment as a reusable stopgap PPE solution for healthcare workers to help address the N95 respirator shortage.
Created: March 19, 2020
Last Updated: May 5, 2020
Documentation License: Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY-NC-SA 4.0)
Short Title: Repurposing of full-face snorkel masks as reusable PPE for healthcare workers
Detailed Title: N95 filter attachment to repurpose full-face snorkel masks as reusable PPE with airborne and splash precautions for healthcare workers.
Technical & Academic Contributors:
- Stanford University Prakash Lab: Prof. Manu Prakash, Laurel Kroo, Anesta Kothari, Thibaut Pollina, George Herring, Ray Chang, Rebecca Konte, Hongquan Li, Hazel Soto-Montoya, Samhita P. Banavar, Elliot Flaum, Grace Zhong, Prakash Lab members
- Melanie Hannebelle, EPFL
- Dominic Peralta, Stellar Design
- Eric Gagner, Boston Scientific
- Olin College of Engineering (Bluetooth App Team): Kyle Combes, Emma Pan, Khang Vu, Kelly Yen
- Deakin University (iOS bluetooth app): James Dale
- Ross Venook, Stanford University Dept. of Bioengineering
- Nicholas Cucinelli, Entrepreneurial Leadership Faculty, U-M
- Rozhin Hajian, Harvard
- Simon Ellgas, Waymo
- Luca Borroni
- Noah Jacobs
- Patrick Gerber, DSPS, EPFL
Clinical Contributors:
- University of Utah School of Medicine: Dr. John Pearson MD, Patrick Kolbay, Dept. of Anesthesiology team
- UCSF Dept. of Anesthesia and Perioperative Care
- Dr. Philip Wagner MD, Hospital for Special Surgery, NYC
- Dr. Roberto Miki, Miami
- Dr. Cristián Muñiz Herrera MD, Chile
- Dr. David Kohn Bitran MD, Chile
- Dr. Peter Baek MD MS, U.S. Anesthesia Partners, Texas
- Nitin Arora M.D., M.P.H, F.A.A.P, Assistant Professor
Children’s of Alabama & University of Alabama at Birmingham
Industry Contributors:
- Boston Scientific: Randy Schiestl, Shannon Abel, Eric Gagner, Darius Mercer, Chase Fetzek, Paul Miller, Martin Plantenberg, Michael Brekke, Tim Dolan, Abigale Bather, Daniel Burgess
- Stellar Design: Dominic Peralta
- Autodesk: CEO Andrew Anagnost
- Wildhorn Outfitters: Gerry Ayala
- Decathlon: Quentin Allinne
- Kober Engineering: Filip Kober
- Dave Kasper, iSnorkel, Inc.
Prototyping, Supply and Manufacturing Partners: FormLabs (Jory Block), PrinterPrezz (Eshaan Gandhi), Origin.IO (Finbarr Watterson), CZ Biohub, Wildhorn Outfitters (Mark Siu and Gerry Ayala), Walmart
Project Leads: Anesta Kothari, Thibaut Pollina and Laurel Kroo
Please write to <manup@stanford.edu> and <pneumask.covid19@gmail.com> if you would like to join our effort.
Project PI: Manu Prakash <manup@stanford.edu>
Document Steward/Editor: Manu Prakash <manup@stanford.edu>
Quick Links:
- Executive summary on Prakash Lab website
- Supplementary document for Pneumask Coupler Design (note: this document is temporarily private for a day to allow for reorganization of document contents)
- Directory of other Prakash Lab COVID-19 response projects
Concept and first functional prototypes currently being tested in the clinic.
Abstract:
A full-face snorkel mask has been adapted and evaluated for use as personal protective equipment for health care workers, who lack appropriate alternatives during the COVID-19 crisis in the spring of 2020. The design consists of a custom snorkel-specific adapter that couples the snorkel-port of the mask to a rated filter (either a medical-grade ventilator inline filter or an industrial filter). Our team refers to this combined solution as Pneumask.
This design has been tested for the sealing capability of the mask, filter performance, CO2 buildup and clinical usability. These tests found the Pneumask capable of forming a seal that exceeds the standards required for half-face respirators or N95 respirators. Filter testing indicates a range of options with varying performance depending on the quality of filter selected, but with typical filter performance exceeding or comparable to the N95 standard. CO2 buildup was found to be roughly equivalent to levels found in half-face elastomeric respirators in literature. Clinical usability tests indicate sufficient visibility and, while speaking is somewhat muffled, this can be addressed via amplification (Bluetooth voice relay to cell phone speakers through an app) in noisy environments. We present guidance on the assembly, usage (donning and doffing) and decontamination protocols.
The benefit of the Pneumask as PPE is that it is reusable for longer periods than typical disposable N95 respirators, as the snorkel mask can withstand rigorous decontamination protocols (including autoclaving). With the dire world-wide shortage of PPE for medical personnel, our conclusions on the performance and efficacy of Pneumask as an N95-alternative technology are cautiously optimistic. The FDA has instructed our industry partners to ship these units as “face-masks” (that may be assembled by healthcare workers themselves and categorized as “improvised” PPE) until they can verify and validate the data and conclusions within this report.
Table of Contents:
Diversity of Full-Face Snorkel Mask
Inhale/Exhale Pathways for the Snorkel Mask
3D Printed Coupler Parts for the Snorkel Mask
Pneumask-G: Anesthesiologist and General-Use PPE
Pneumask-S: Surgeon-Specific PPE
Testing and Ongoing Clinical Validation
Evaluating Potential Leakage from Chin Valve
Valve Closure Times Estimation
Exercise test
Simulation of CO2 Species Transport and Flow Modeling (CFD)
Improving Communication Through Mask
Decontamination Protocol Testing
Failure Modes and Effects Analysis (FMEA)
Estimated Benefit of Pneumasks during Mask Shortages
Forking and Working Independently
Appendix A. Supplementary Tables
Appendix B. Suggested Decontamination Protocols
Cleaning and Decontamination Protocol (Not an Approved Protocol)
Appendix C. Communication App User Instructions
Appendix D. Suggested Donning/Doffing procedures
Appendix E. Supplementary Figures
Description of Innovation
Personal protective equipment (PPE) is one of the most important protective layers for healthcare workers around the world in a crisis like COVID-19 [1, 2]. However, the supply of PPE in hospitals is at an extreme low and is rapidly depleted by the day [2-4], while the industrial supply chain is unable to scale up to meet current demands [5]. Our proposed Pneumask is a potential stop-gap kit-of-parts solution consisting of an off-the-shelf snorkel mask, a custom (3D-printed / injection-molded) adapter, and a filter/filter cartridge. The primary benefit of a snorkel mask is providing a full-face shield and air seal while allowing for controlled intake and exhaust flows through the mask. Such masks are already widely available in large quantities and tapping into their supply chain would allow their production to be quickly ramped up during this crisis. On each typical mask is a ventilation port consisting of 1 inhale and 2 exhale channels, located at the top of the mask (Figure 1). In most models, there is an additional exhale port toward the mouth/chin area, which can be easily blocked. The full-face shield has been tested to withstand disinfection protocols, which may include a 30-minute autoclaving cycle or a simple 2-minute bath in 50ppm chlorine solution, while still maintaining its seal performance after the disinfection. This would allow the masks to be reused overtime.
Our designs are aimed specifically at doctors, nurses and hospital staff (specifically for use in settings where no alternative FDA-approved medical PPE is available or suitable for use). Unlike many other open-source designs that are intended for ventilated patients or consumers, this mask is primarily designed to prioritize the protection of a healthy user, rather than the surrounding environment. It is assumed that users are alert and active during mask usage, can be trained on standard operating procedures, and have access to standard sterilization and disinfection methods used in hospitals.
The goal is to connect this ventilation port to a filter via a custom 3D-printed adapter. There are a couple of strategies with regards to the filter: (1) use off-the-shelf breathing circuit filters, which can be include viral filters (housed in factory-standard cartridges) rated at 99.9% effective for blocking 0.1um or above and can be directly connected to the adapter, or (2) use alternative filter materials, such as HEPA filters, that can be housed in a custom 3D-printed cartridge which connects to the adapter. (A complete list of ventilator inline filters and industrial-used filters that may be used for this application is listed in Appendix A Table 1 and Appendix A Table 4.) Both approaches to the filters include a durable cartridge, which allows for a longer life-span of the filter material as compared to the standard N95 respirators.
Pneumask can provide a much safer solution to the current PPE shortage crisis compared to untested homemade masks or bandana, which cannot provide perfect seal around the face and are not tested for filtering efficiency. Pneumask can also be usable for surgeons who fail N95 fit tests as they cannot use any positive air pressure respirators while operating over a surgical field as long as the front one-way valve is sealed.
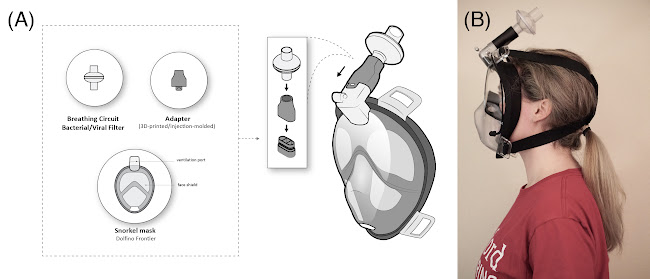
Figure 1: (A) Proposed Pneumask and (B) Prototype pictured on user. The snorkel mask is connected to an inline viral filter to provide protections to healthcare workers. The snorkel mask and adapter can be disinfected thus provide a reusable solution.
Design
Diversity of Full-Face Snorkel Masks
Today a huge diversity of full-face snorkel masks are commercially available (Please refer to and Appendix A Table 3 to see the list of commercially available full-face snorkel masks or inspect this complete table here). The original concept for these masks came from the Subea Team (Figure S1). Subea has generously provided us a CAD file of their mask which enables a precise manufacture of an adapter. Additionally, we have also developed (reverse-engineered) the geometry of the connecting feature and the CAD adapter for the Dolfino Frontier mask, which is openly available. We have focused our design effort in this document specifically on the Dolfino Frontier mask unless otherwise stated.
Inhale/Exhale Pathways for the Snorkel Mask
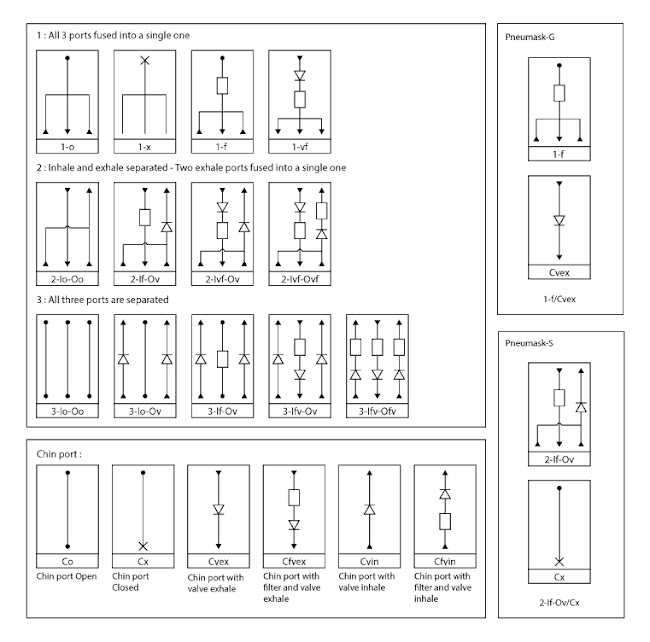
To facilitate further design and communications, we have developed a standard nomenclature for possible connection configurations of a snorkel mask (Figure S6) and convert the air flow pattern of a non-modified snorkel mask (Figure 2A) into an airflow diagram like Figure 2B. In the normal mode of operation of a non-modified snorkel mask, the inhaled air passes through the center channel of the snorkel, enters the eyes chamber, then the mouth chamber, and is inhaled by the user. In water, the chin valve is blocked, and all the exhaled air goes through the two side channels of the snorkel. In air, most of the exhaled air goes through the chin valve. Both in air and in water, the inhale and exhale paths are separated.
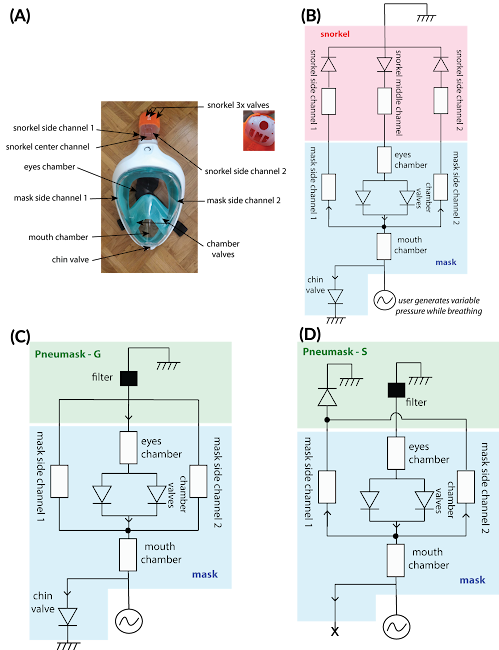
Figure 2: (A) & (B) Air flow pathways of the snorkel mask (based on Decathlon Easybreath), (C) Pneumask-G and (D) Pneumask-S. Notation: diodes=valves; ground=atmospheric pressure.
Coupler Parts for the Snorkel Mask
With aids of the airflow diagram, our team currently has 2 designs of the coupling adapters that are targeted at two different use cases. Older designs from our team, and design efforts from other groups we are aware of (including adapters for mask styles other than the ‘Dolfino Frontier’ mask) are documented in a supplementary document.
- ANESTHESIOLOGIST AND GENERAL-HOSPITAL USE PPE: The first, most prevalent use-case is a PPE solution for hospital personnel that do not require a “sterile-field”. Functionally, this means that the air exhaled by the user does not need to be filtered, or redirected away from the patient. This use-case is the application for the majority of the workers in hospitals. We will refer to this prototype in this document as “Pneumask-G”. (Figure 2C)
- SURGEON PPE: The second design is specifically targeting the needs of surgeons (a vast minority of the use-cases), which has filters on both the inhale and the exhale, and directs the exhale away from the patient. We will refer to this prototype in this document as “Pneumask-S”. (Figure 2D)
Pneumask-G: Anesthesiologist and General-Use PPE
In Pneumask-G, the airflow is designed such that all inhaled air is through filter(s) attached to the top of the mask, and exhale is all through the built-in 1-way valve at the chin of the mask (Figure 2C). This design of this main system is modular to allow adaptation to supply chain shortages of filters. It consists of 2 custom adapters:
- An adapter that interfaces the Dolfino Frontier full-face snorkel to a female filter port, designed to accept an ISO standard 22mm OD viral filter (Figure 3B). This adapter connects the snorkel to a single standard respiratory filter that is already in supply at many hospitals. Some images of these filters are provided below. Only air from inhale is meant to be channeled through this adapter. An optional one-way valve can be placed between the adapter and the filter to prevent any exhaled air from going back to the filter, which lowers fogging and CO2 buildup. Optional valve and air pathway modifications are discussed in the coupler design supplementary. The final coupler that Eric Gagner of Boston Scientific designed can be downloaded here (.STEP only): https://www.dropbox.com/sh/sztddvy1or1auc7/AABI99D3pklqkQBGL7xdTKHNa?dl=0
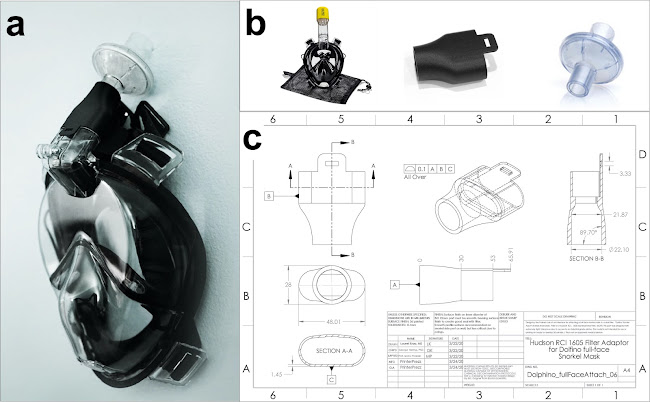
Figure 3: (A) This is the first solution that enables use of a snorkel mask to be used as a full reusable PPE; including (B, from left to right) Dolfino full face snorkel mask, an adapter, and a Hudson RCI 1605 inline filter. (C) The design is based on the connector standard ISO 5356-1:2015 Anaesthetic and respiratory equipment - Conical connectors - part 1: Cones and Sockets). A newer version of this part was adapted for use with injection molding by Boston Scientific.
The configuration of the Peumask-G design shown in figure 3A can be implemented with any rated filter with an ISO 22mm OD port. This includes both HME filters (some of which are HEPA-rated) and viral filters. The performance of the design in terms of 1) work of breath and 2) CO2 accumulation will depend on the filter that is used inline in the system. Performance was adequate with most filters that we tested (see more in testing section); air-pathway modifications (such as blocking the side exhale channels) are not strictly necessary, but can improve comfort.
- In the case of supply shortage of the respiratory filters, there is a second adapter piece that we’ve designed to replace the viral filter with two P-100 filters made by 3M (Figure 4a). This adapter interfaces with the snorkel-to-ISO part, and can be added onto the prototype. The input port is a male ISO standard 22mm. The output port is designed to connect to standard cartridge filters by 3M. Two gaskets are required to mount these filters (Figure 4b), and typically must be ordered separately. The validity of using P100 industrial filters for infection control is first provided by Gardner et al [15], in which they tested the viral penetration through an N95 and P100 respirator, and showed that those respirators filtered out viral particles as they claimed filtering efficiency. At the same time, we are also repeating the tests and will share the results soon.

Figure 4 (a) Part Design of a male 22mm ISO to two standard ¼ turn socket ports for industrial-grade filters. (b) Assembly with two P100 filters (Part 2097, 3M), (c-d) Mask assembly with multiple types of industrial NIOSH filters. (e-f) Full assembly on Dominic Peralta with different filter types. A complete list of possible industrial filters that can be potentially used are provided in Appendix A Table 4.
Pneumask-S: Surgeon-Specific PPE
This design was recognized as an important, separate challenge with regards to the specific needs of hospital personnel that are required to perform ‘sterile-field’ procedures. During surgical procedures, the air exhaled by the surgeon must be directed away from the patient; and preferably be filtered [16].
The chin valve can be modified to be permanently closed/blocked for this prototype (Figure 2D), such that all exhaled air is ported through the two outside channels in the top of the snorkel. A single-part design has been developed for connecting the center channel of the snorkel (for inhale) to a male filter port, and the 2 outside channels (for exhale) to a separate male filter port. This design has the benefit of fully separating the input and output streams, while avoiding use of the chin valve. A one-way valve on the input prevents any exhaled air from going back to the filter, and lowers fogging and CO2 buildup (optional). The exhale port needs to be connected to a one-way valve (mandatory).
Testing and Ongoing Clinical Validation
The primary function of a respiratory protection is to protect the wearer from exposure to pollutants present in air, currently from particles exhaled/sneezed/coughed by an infected individual. The residual exposure of the wearer depends on three independent additive components: the leak at the face, the penetration through the filter and the internal contamination.
Residual exposure = leak at the face + penetration through the filter + internal contamination
The leak at the face depends on how well the mask forms a seal with the wearer face, or said differently how well the mask fits the wearer face. The fit is clearly dependent on the mask shape and the morphology of the individual face, and should be determined systematically for each wearer with each of the mask models used. As the origin of the leaks is a breakthrough in the sealing, the fit is considered independent from the nature of the pollutant.
The penetration through the filter depends on the efficiency of the filtering material to remove particles from the air. The filtration efficiency is clearly a characteristic of the material and the natures of the particle, and is independent from individual and from the mask shape. The filtration efficiency has to be measured under normalized conditions, or at least with well characterized particles corresponding to the pollutant the wearer has to be protected from.
The internal contamination is mainly due to an inadequate maintenance of the mask, but could be significantly reduced by wearer training, adapted maintenance, and storage protocols (such as sterilization).
Currently, the particles exhaled by the mask wearer have the same size range as these generated by the patients, and which the mask should protect against. This means that the global protection factor of the mask concerning these specific particles cannot be determined while the mask is being worn, as the wearer-exhaled particles will be misinterpreted as a leak. Thus, the fit and the filtration efficiency have to be determined separately. The exposure of the wearer will be considered under control when both fit and filtration efficiency criteria are respected.
Fit Test & Seal
For their intended purpose, the seal tests of snorkel masks are done by the manufacturing companies underwater. However, the sealing ability of the snorkel masks on dry skin is unknown. Per CDC and NIOSH regulations on the use of elastomeric respirators, a fit test can be performed in the same manner as N95 respirators to ensure seal and safety to use for an individual [19]. At this time, we recommend that all practitioners seeking to utilize these masks perform a fit test under standard N95 fit test conditions.
In addition to this recommendation, additional fit test experiments have been performed in our laboratories. Practically, two types of fit test can be conducted:
- Qualitative fit test: a liquid aerosol with a sweaty or bitter taste are generated within a confinement around the head of the mask wearer. The result of the fit test is based on the detection of the taste under the mask.
- Quantitative fit test: the method is based on a particle counting outside and inside the mask in parallel using the TSI Portacount device. The ratio out/in gives the fit factor.
Qualitative Fit Test
At the University of Utah, we performed a qualitative fit test on 3 separate volunteers, utilizing our 3D printed adapter and both an HME anesthesia circuit filter and a HEPA anesthesia circuit filter on a Dolfino Frontier mask (Figure 5). Out of 3 volunteers, 2 were male and 1 was female, and both males had failed their fit test in the past using regular N95 respirators. The fit test was performed by the standard University of Utah Operating Room team as for N95 tests, as part of the emergency COVID-19 response in order to evaluate emergency countermeasure personal protective equipment. Importantly, all 3 individuals passed their fit tests. This preliminary result seems to indicate that the fit seal satisfies the minimum requirements for an N95 respirator or elastomeric respirator.
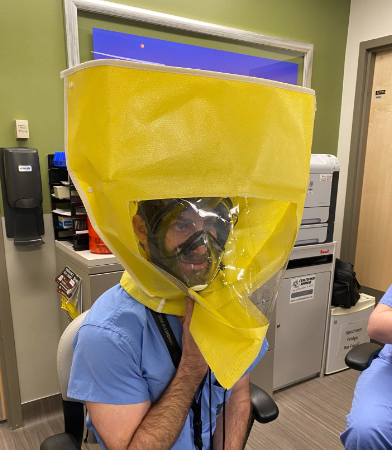
Figure 5. A qualitative fit test was performed by the standard University of Utah Operating Room team using the same protocol suggested by CDC and NIOSH on elastomeric respirators and N95 masks.
Quantitative Mask Performance
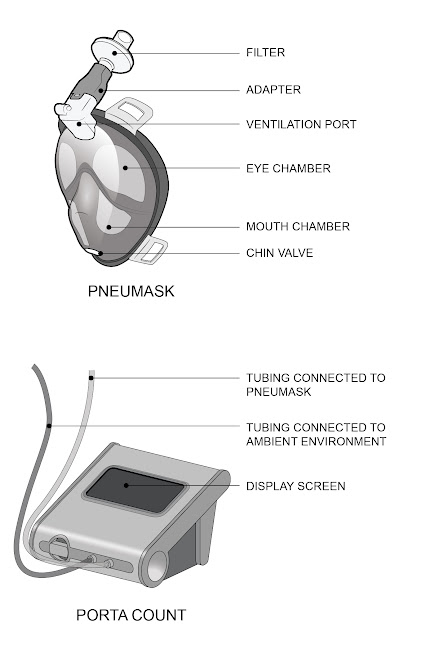
Figure 6. Pneumask and PortaCount essential components
Mask Fit
The fit test is only meant to measure the ability of the mask to form a seal with the wearer's face, and not the efficiency of the respiratory protection. The principle of this test consists of successive measurements of the particulates concentrations inside and outside of the mask during normalized exercises. The ratio between the external and the internal concentrations is called fit factor (FF). The relevancy of the results is dependent on a few assumption:
- The efficiency of the filter is high enough to assure that the particle penetration rate is insignificant compare to the expected leak rate, within the range of the measured particle size (0.015-1 μm). P3, N100 or HEPA filters are generally used (filtration rate >99.95% at 0.3 μm) to reach this specification, with a theoretical FF > 2000 in case of perfect fit. For filters with significant penetration rate (P2 or N95), the measure is based on smaller subset of particle sizes (around 0.04 μm) using the N95 protocol to avoid the counting of the filter-penetrating particles.
- The range of the particle size measures by the Portacount (0.015-1 μm) has been selected to stay mostly outside of the range of particulates generated by human exhalation, apart from smokers who have to stop at least 30 minutes prior to testing. This is necessary because the particulates generated by mask wearer would otherwise be misinterpreted as a leak into the mask.
- The ambient particle count exterior to the mask, in the particle size range measured by the machine, must be significantly higher than the quantity of particles that could be generated by the wearer by any method. The Portacount stops automatically the measures if the particle rate decreases under a minimum level.
Practically, the quantitative fit test will not measure only the leaks at the wearer’s face, but also any leaks in relation with the connection after the filter or with the exhaust valve. In this way, high fit factors will not mean only that the leaks at the wearer’s face are acceptable (wearer dependent), but also that the residual leaks at the level of the new 3D designed connector and the chin valve are under control (wearer independent).
Experiment Parameters
- Fit measured using a Portacount Pro+
- OSHA Standard
- Half Mask protocol (non-N95)
- 4 candles to provide a constant ambient particle source
- Test Subject: 28 year old male, no facial hair, no history of smoking
- HME HEPA filter (Pall Ultipor 25)
- Snorkel Mask (Dolphino or Decathlon)
- Modified adapter from Formlabs high temperature resin

Figure 7. Modified adapters with tube connectors
In order to collect a thorough measurement, each test was repeated three times, sampling from the mouth chamber, the eye chamber, and directly from the adapter, right after the filter. This required building two modified adapters. The adapter which sampled directly after the filter was modified by drilling a hole in the adapter between the filter connection port and the mask port. The drilled hole was cleaned and smoothed before a luer lock connector was press fit into the hole and sealed using epoxy. The epoxy was allowed to cure for 24 hours and the assembly was subsequently washed with isopropyl alcohol for 2 minutes. The adapter which sampled from the eye chamber and mouth chamber used a flexible tube to sample air from a desired location. This adapter was modified by drilling a hole large enough for the flexible tube to pass through. The hole was once again cleaned and a luer lock connector was pressed into the tube. The luer lock connector and tube were press fit into the drilled hole and sealed using epoxy. The epoxy was allowed to set for 24 hours before the entire assembly was washed for 2 minutes in isopropyl alcohol. Both adapters were allowed to dry completely before any tests were conducted.
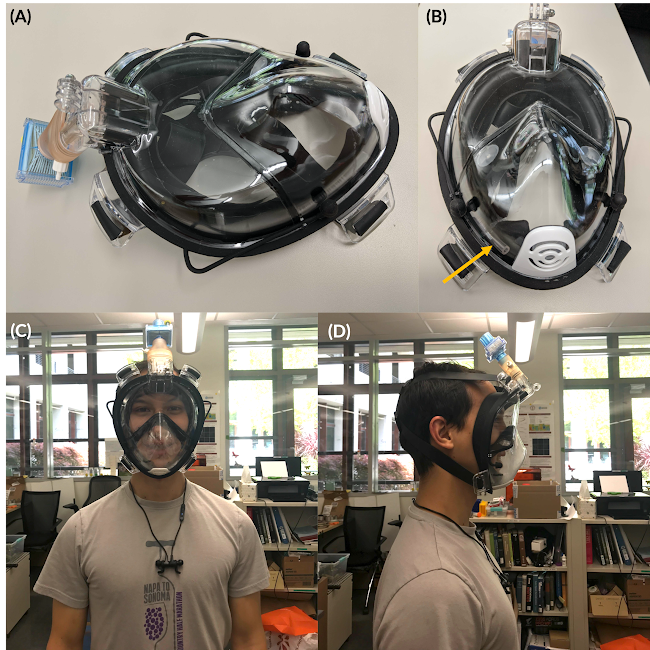
Figure 8. (A) Modification of adapter for quantitative fit test. The sampling of the air inside the mouth chamber is achieved by a flexible tubing running through the side channel and connected to the sampling port on the adapter. This method avoids possible destructions on the mask surface. (B) The yellow arrow points out the tip ending of the sampling tube. (C) The front view and (D) side view of our testing subject wearing the mask.
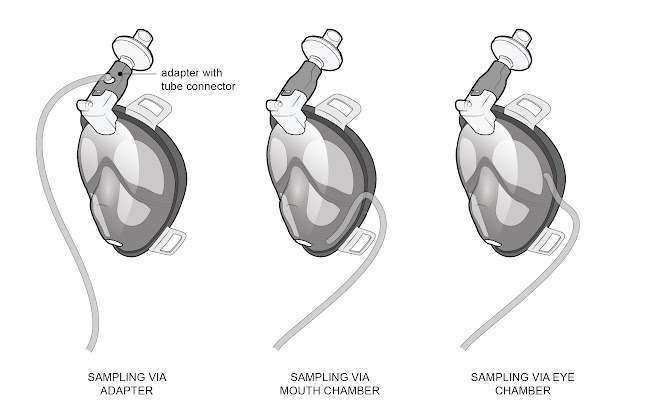
Figure 9. Different testing methods/measuring locations
Dolphino Experimental Results
Mouth Chamber | Eye Chamber | Inlet Port | |
Normal Breathing | 482 | 291 | 2713 |
Deep Breathing | 133 | 194 | 1209 |
Head Side to Side | 439 | 255 | 2766 |
Head Up and Down | 257 | 230 | 1471 |
Talking | 360 | 173 | 698 |
Bending Over | 1104 | 509 | 3020 |
Normal Breathing | 477 | 568 | 2766 |
Overall Fit Factor | 325 | 266 | 1605 |
Further tests were completed independently at Stanford Occupational Health and Safety which confirmed that the dolphino mask passes the quantitative fit test.
Table 3. Results of quantitative fit tests using PortaCount 8048, conducted by the EH&S team at Stanford Health Care. The sample is obtained from the adapter site, using a modified adapter as shown in Figure 8.
Respirator: Pneumask-G using Dolfino Frontier L/XL Model: Full Face | Protocol: OSHA Fast-Full/Half Face Pass level: 500 | ||
Exercise | Duration (sec) | Fit Factor | Pass |
Bending over | 50 | 784 | Y |
Jogging in place | 30 | 1152 | Y |
Head side to side | 30 | 944 | Y |
Head up and down | 30 | 1042 | Y |
Overall FF | 961 | Y | |
Two additional fit tests were conducted at Stanford Environmental, Health and Safety – one completed using the requirement of a half-face elastomeric respirator and another using the fit factor for a full-face tight fitting Air Purifying Respirator, and the results are shown in Table 3. The participant (female) wearing Dolfino Frontier with a custom adapter, and a Pall Ultipor 25 breathing filter, who is typically a size M, was still able to pass the quantitative fit test well beyond the requirements on both tests. The minimum passing fit factor was 100 for half-face respirator and 500 for a full-face respirator. The activities that were tested while wearing the mask included bending over (50 seconds), jogging in place (30 seconds), moving head side to side (30 seconds), and moving head up and down (30 seconds), and the fit factor outcomes were all above 750. Please note that, although the test yielded positive results, this was conducted with a limited testing sample and does not yet indicate any certification/endorsement from EH&S of the product. Each entity should also conduct its own evaluation and testing before use.
Subea Decathlon Experimental Results
Mouth Chamber | Inlet Port | |
Normal Breathing | 134 | 139 |
Deep Breathing | 120 | 117 |
Head Side to Side | 127 | 98 |
Head Up and Down | 104 | 78 |
Talking | 111 | 116 |
Bending Over | 94 | 170 |
Normal Breathing | 90 | 142 |
Overall Fit Factor | 110 | 116 |
Important Note: The couplers used in the above test did not fit the Subea mask as well as the Dolphino mask. Tape had to be used to form a better seal. Thus these results should be interpreted as a lower bound on the sealing capabilities of the mask.
Person | Date | Size Mask | Valves Between Eye and Mouth Region | Filter Type | Test Protocol | Overall external / internal report |
Apr 9, 2020 | M/L | Closed (stock configuration) | HME | N100 | 4 (N100 test protocol not suitable for HME filter) | |
Person 1 | Apr 9, 2020 | M/L | Closed (stock configuration) | HME | N95 | 200+ |
Apr 9, 2020 | M/L | Open (mouth and eye regions connected) | HME | N95 | 200+ | |
Apr 9, 2020 | M/L | Open (mouth and eye regions connected) | HME | N100 | 4 (N100 test protocol not suitable for HME filter) | |
Person 2 | Apr 9, 2020 | M/L | Open (mouth and eye regions connected) | HME | N95 | 200+ |
Apr 9, 2020 | M/L | Open (mouth and eye regions connected) | HME +P3 | N100 | 163 |
Validation of the fit of the Decathlon mask was completed in a separate series of experiments also using a Portacount Pro+ in N95 mode and following the OSHA 29CFR1910.134 protocol. The Decathlon Easybreath mask was connected to a medical grade HME filter (DAR adult-pediatric electrostatic filter HME, small) with a 3D-printed PLA connector. The mask was in Pneumask-G configuration (3 snorkel ports connected to the filter, chin valve non modified). The mask was connected through the silicon skirt of the eyes chamber, as indicated on the picture below, using the standard connector sold by the manufacturer of the particle counter. In N95 mode, the test was positive for the two individuals (men, freshly shaved) tested, with a fit factor of 200+, which is higher than the requirement for half-masks (100). Removing the chamber valves to connect permanently the eye chamber and the mouth chamber led to the same results. This test was run in N95 mode because the test was completed using an HME filter which was not HEPA rated (fit factors around 4 would have been obtained with the N100 normal protocol under the same testing conditions).
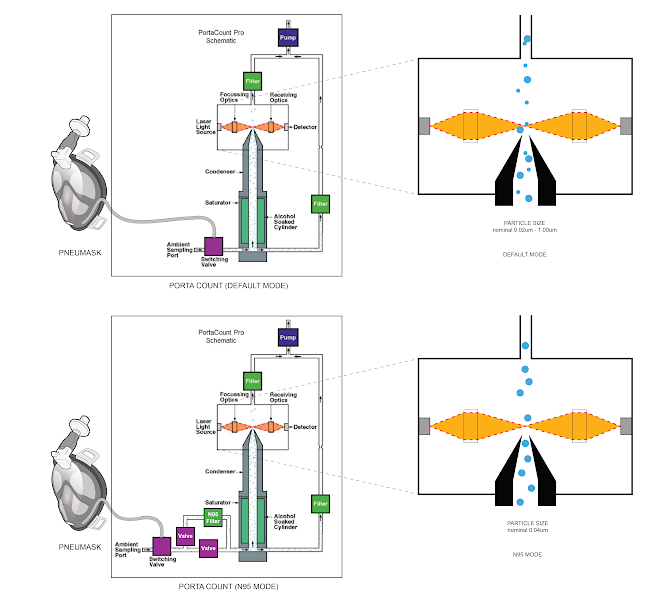
Figure 11. Difference in PortaCount’s functionality across the default and N95 modes.

Summary of Findings
The successful results for the fit test with the different individuals used in this study indicate that the Dolphino and Decathlon masks both form acceptable seals, showing also that the 3D printed connector and the chin valve do not generate significant leaks. The measured fit factors correspond to the requirement for elastomeric half-mask. The remaining performance of the mask depends on the efficiency of the filter, which is attached to the mask.
The position of the sampling point gives similar results between the mouth and the eyes chambers. However, a sampling point directly connected on the 3D printed adapter shows significant higher fit factors, which seem over evaluated, probably due to the proximity of the filter. In this case, the measured particle concentration should not be relevant of the real concentration in the breathed air.
The use of the N95 protocol of the Portacount is important for the fit evaluation when HEPA filters are not available, especially with HME virus filters. The efficiency of the filters have to be measured independently to assure safe working conditions.
Mask Filtration
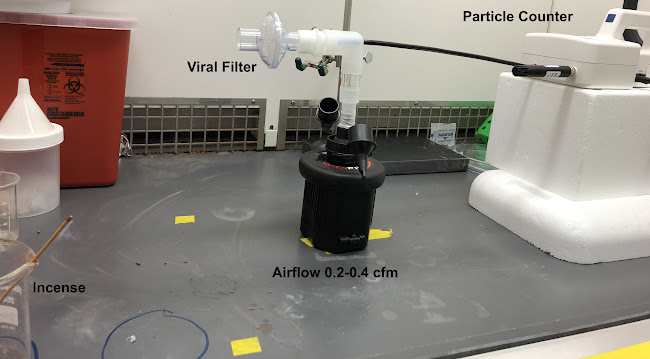
Figure 13. Setup for measuring filter efficiency.
We developed an experimental test rig and method for testing the particle filtration efficiency of various materials including N95-grade masks. The setup pictured in figure 13 includes a LightHouse handheld particle counter (Model 3016 IAQ), Intex QuickFil 6C Battery Pump, a rubber stopper with 2 holes covered by 2 kim wipes to mitigate the airflow, Incense: Satya Sai Baba Nag Champa 100 Gram, connectors (universal cuff adaptor, teleflex multi-adaptor), and filters to test (Hudson RCI Main Flow Bacterial/Viral Filter, Romsons HME Disposable Bacterial Viral Filter, Pall Ultipor 25 filter). The pump with the rubber stopper, covered by 2 kim wipes, in it, provides an airflow within a range of 0.2-0.4 cfm to mimic that of breathing. The incense produces particles of various sizes, including those in the range picked up by the detector (0.3 µm - 10 µm). With the pump on, we measure the number of particles produced by the incense. Then we place the filter on the setup and run the particle counter to measure the number of unfiltered particles. To calculate the filtration efficiency, we calculate the ratio of unfiltered particles to the number of particles produced by the incense, and then subtract from one. The filter efficiencies for the 3 filters tested are reported in table 3.

Figure 14. Variety of filters tested.
Table 3. Filter efficiency and pressure drop across filters
Filter | Filter Efficiency of particles sized 0.3-4.49 µm for airflow rate of 2.83 l/min | Filter Efficiency of particles sized 0.3-4.49 µm for airflow rate of ~8.5 l/min | Pressure drop across filter for airflow rate of ~6.0 l/min |
Hudson RCI Main Flow Bacterial/Viral Filter | 99.67% ± 0.26% | 97.71% ± 1.07% | 16.11 ± 1.95 Pa |
Romsons HME Disposable Bacterial Viral Filter | 99.83% ± 0.04% | 97.97% ± 0.43% | 18.31 ± 2.37 Pa |
Pall Ultipor 25 filter | 99.88% ± 0.04% | 99.98% ± 0.00% | 24.20 ± 4.23 Pa |
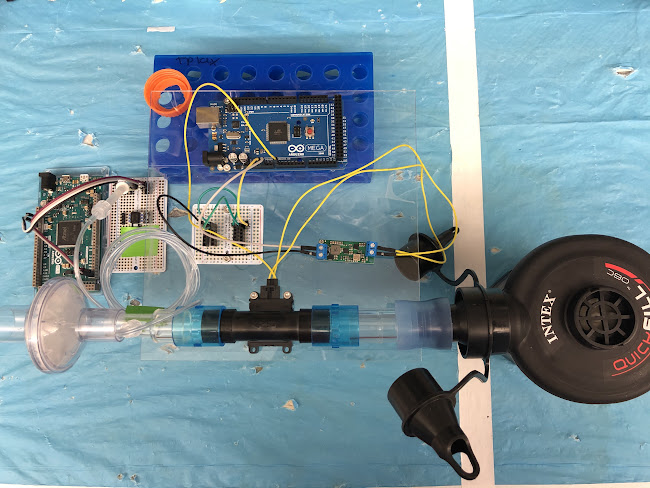
Figure 15. Setup for measuring pressure drop across filter.
We constructed an experimental system for measuring the pressure drop across various materials, including N95 masks, during inhalation and exhalation. The setup in picture figure 15 includes an Intex QuickFil 6C Battery Pump, a Honeywell AWM700 Airflow sensor, a Honeywell ABPDLNN100MG2A3 Pressure Sensor,a rubber stopper with 2 holes covered by 2 kim wipes to mitigate the airflow, connectors (universal cuff adaptor, teleflex multi-adaptor), and filters to test (Hudson RCI Main Flow Bacterial/Viral Filter, Romsons HME Disposable Bacterial Viral Filter, Pall Ultipor 25 filter). The pump with the rubber stopper, covered by 2 kim wipes, in it, provides an inhalation or exhalation airflow within a range of 0.2-0.4 cfm to mimic that of breathing. With the pump on, we measure the airflow applied to the mask, and the differential pressure drop across the mask. The pressure drops for the 3 filters tested are reported in table 3.
Summary of Findings
Pull Test (Adapter-to-Port Seal)
To determine the potential for breaking of seal in the snorkel mask to adapter coupling, we tested the linear pull force necessary to disconnect adapter/O-ring male mask coupling on a BodyGlove snorkel mask. We found this force to be 17lbs, which was the same as for the supplied snorkel, and compared favorably with our measured linear linear pull force necessary to disconnect the 22mm male ISO adapter/female ISO Virex filter coupling of 9lbs.
Evaluating Potential Leakage from Chin Valve
Exhalation Valve Leakage Test (NIOSH Standard)
One concern our team had was the ability for particulates to enter through the chin exhalation valve. As these snorkel valves are not medically approved, it is necessary to understand the performance of the valves to assess safety. The NIOSH standard “Exhalation Valve Leakage Test” (Section 84.182) stipulates the pressures and flow rates necessary for equivalent performance standard to typical N95 respirators. Particularly, it states that: “(a) Dry exhalation valves and valve seats will be subjected to a suction of 25mm water-column height while in normal operating position. (b) Leakage between the valve and valve seat shall not exceed 30 milliliters per minute.” [28]
With this specification in mind, we conducted the following test to determine technical equivalency to NIOSH for this sports equipment to safely stand-in for a medical device.
A chamber was glued around the chin valve using epoxy, and an 8mm tube was connected to this chamber (Figure 8A). The 8mm tube is connected to an opened water tank (Figure 8B).
First, the water was allowed to equilibrate by manually opening the chin valve briefly (Figure 8B). Then, the mask was lifted up to create a water column of 30mm (Figure 8C), which corresponds to a negative pressure of 30mmH2O applied to the chin valve. As time passes, the small leakage of the chin valve reduces the negative pressure and therefore the height of the water column.
The leak of the chin valve can be approximated as the ratio between the volume of air in 10mm of tube length, and the time it takes for the water column to go from 30mmH2O to 20mmH2O. We measured the leak of the chin valve for 5 different valves, for pressures ranging from -15mmH2O to -145mmH2O (Figure 8D). NIOSH regulation specifies that the maximum acceptable leak rate for an exhale valve is 30mL/min for an applied pressure of -25mmH2O. The average leak rate for the 5 valves was 4.2mL/min at -25mmH2O, and the maximum flow rate at -25mmH2O was 15.8 mL/min. We conclude that the leak flow of the exhale valve (chin valve) is lower than the maximum flow allowed to comply with the NIOSH regulation (30mL/min for -25mmH2O of pressure). It is noted that this test was done on a specific mask model our team had available, the Decathlon EasyBreath.
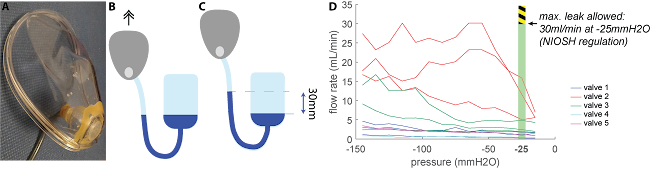
Figure 8. Setup for measuring the leak flow of the chin valve of a Decathlon EasyBreath mask. (A) Connection to an 8mm tube. (B) Connection to an open water tank - system at equilibrium (chin valve opened). (C) The mask is lifted up (chin valve closed) to create a water column of 30mm, which means that a negative pressure of 30mmH2O is applied to the chin valve. (D) Flow rate through the chin valve as a function of the applied pressure. 5 different valves were tested; for all valves, the leak rate was well below the maximum value allowed by NIOSH regulation (30mL/min at -25mmH2O of pressure). Valves 1-3 were used for at least 10 minutes before the measurement, valves 4 and 5 were new.
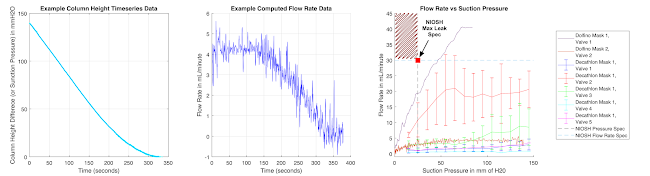
Figure 9: Leak Flow Rate Test Results for two dolfino masks were 19.3 mL/minute and 3.06 mL/minute at a suction pressure of 25 mmH2O. This is better than the NIOSH requirement. Plot on the far left is the experimental data as a time series of the column height (suction pressure). Middle plot shows the flow rate as a function of time (example of one dataset). Far right plot shows the flow rate as a function of suction pressure (note that this plot has a flipped x-axis relative to figure 8d. NIOSH Specifications are indicated on the plot.
Next, we did these same tests for the Dolfino Frontier mask, as shown in Figure 9. The experiment was identical to the experiment shown in panels b and c for Figure 8. However, for the Dolfino Frontier, we extracted quantitative data on a high-resolution video through image-processing, rather than using an approximation. Panel A of Figure 9 shows the time series of the column height difference. We then computed the flow rates associated with the suction pressures at each frame of the video. The dolfino valve leak rates were 19.3 mL/minute and 3.06 mL/minute mL/minute at a suction pressure of 25 mmH2O for 2 different brand-new masks (with valves in stock configuration and no pieces removed). This is below the maximum flow rate of 30 mL/min that is stipulated by the NIOSH standard. We are working on expanding figure 9 to include results from more Dolfino masks to add robustness to this data, which suggests that valve performance is sufficient for this application. Data from Decathlon masks are also shown in figure 9c for comparative purposes. The two brands seem to behave roughly similarly, and both models consistently perform to NIOSH spec.
Using one of the Dolfino masks (that easily passes NIOSH-spec with a dry, new valve), we also collected quantitative data on the performance of the valve after 30 minutes of a user wearing the mask. As many early qualitative tests showed, the data in figure 10 shows that the presence of humidity appears to decrease the leak rate slightly. It is noted that the NIOSH spec specifically stipulates dry-valve testing; so we caution readers not to use any of the used-mask data in Figure 10 to directly compare to the NIOSH standard, as it would be overly optimistic.
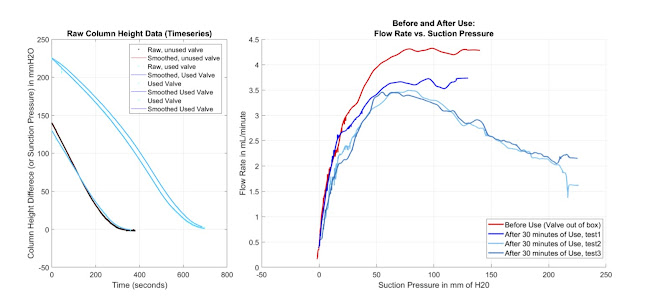
Figure 10: Leak Flow Rate Test Results for a Dolfino Frontier chin valve before and after 30 minutes of use. The left panel shows the raw data from the 4 tests (1 on a new mask and the following 3 on the same mask after usage). It is noted that different tests started at different column heights. The right panel shows the flow rate as a function of suction pressure, similar to panel C of figure 9. However, the blue lines were directly after use. As we have seen on several masks, the data shown here indicates that the valve performance is not decreased by use.
We encourage any readers who are interested in replicating this work (on these masks or on other mask brands) to consider using this water-column based approach for valve testing, rather than air vacuum-based experimental systems that use compression pumps. Highly volatile airflow that is generated in air-based vacuum pumps may cause local perturbations in pressure at the valve that could interfere with clean measurements. It is noted that the tests performed in figures 8, 9 and 10 are destructive to the masks, as they require extensive epoxy or sealant on the connection between the suction tube and the interior of the mask. If readers wish to replicate these experiments (either on these same masks or on other mask brands), please be aware that the seal between the interior of the mask and the suction tube is extremely sensitive and prone to leaking itself. This sensitivity comes from a mechanical issue with the connection: the region that one is sealing to is geometrically complex and there is no easy “seat” for the connector to lock into. Leaks in the experimental set-up will falsely generate very poor performance tests; so please run controls on the system to verify that indeed the measurement system is not flawed. One such control is to hold or tape the valve closed physically while a suction pressure is applied via water-column; there should be no noticeable motion at all in the column over a long period of time (5+ minutes). Additionally, take care to keep the valve seat completely dry in this test; this is a requirement of the NIOSH standard. The use of additional sealant (such as vaseline) over the top of the epoxy connection may improve the measurement system seal further, if your connection is sensitive. With regards to valve failure testing (such as exposure to disinfectants, or exposure to cycles of user-testing as in figure 10), always verify the quality of the measurement system ( seal to the valve) prior to each test.
We do caution readers that valve performance may be mask-brand dependent. The tests in figures 8 and 9 verify valve performance only on two brands (Decathlon EasyBreath and Dolfino Frontier), with a relatively small sample size. We expect some brands of masks might fail these tests.
Additionally, valves should be carefully inspected on individual units prior to use, to make sure manufacturing error or scratches are not present in functionally-critical places (such as the seat of the valve, or on the elastomeric valve piece). Mask brands that use elastomeric valves manufactured through higher-tolerance industrial fabrication methods will likely have far superior performance. We suspect some mask brands use a liquid injection molding rather than a compression molding for these soft elastomeric structures. Liquid molding is a better technique to achieve high precision on such thin and sensitive structures. Scratches on the valve seat or molding errors due to aging injection-molds could possibly cause some individual units to fail, even on the brands we have verified. So we urge users to carefully inspect each unit’s chin valve, and proceed cautiously despite our findings.
A quick fit test by the user can be a good way to check there is not something obviously malfunctioning with individual units. This can be done by assembling the Pneumask, and sealing the top port tightly (with a hand or by some other means), while trying to inhale (holding a suction pressure). The mask will suction up against the face. Because air should only be able to enter through this top (sealed off) port, malfunctioning valves may be identified if there is a hissing or flapping noise that is identified in this situation. There should be no noticeable leaking and no noises coming from the individual mask unit. Do not use any individual unit that hisses or noticeably leaks in this test; consider any such unit as expired, and discard.
Valve Closure Time Estimation
Aside from the above testing, we had also done the following calculation to see how long the chin valve closes (Figure 10 A, Figure 11), assuming standard exhale, to assess the likelihood of backflow. The following figure (Figure 10 B) shows the schematic of a circular chin valve, which is pinned at the center. The valve is assumed to open from the bottom side, moving from vertical position to an angled location after exhalation of air.
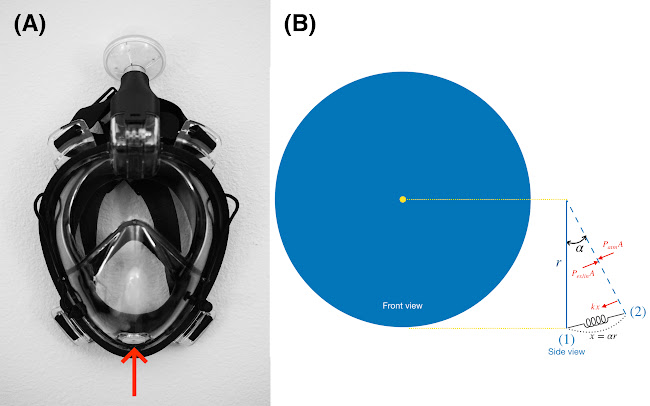
Figure 10: (A) Chin valve on mask, (B) Schematic of a circular chin valve
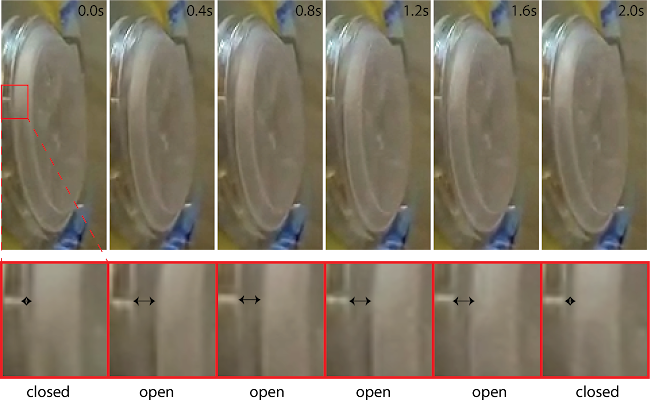
Figure 11: Time-lapse images of the chin valve opening and closing
Forces acting on the valve include the force due to the gauge exhale pressure, ( =
= ), and elastic forces. The elastic force occurs to return the valve to its original shape, this force is simply modeled by a linear spring formula.
), and elastic forces. The elastic force occurs to return the valve to its original shape, this force is simply modeled by a linear spring formula.
These forces should balance for a static valve at (2):

where A and k denote the cross-section area and the elasticity constant of silicon, respectively.
Now, let's assume inhale starts at time t=0 and valve is in the angled position (2) shown in Fig. (10 B),  . At each time instant, in addition to the elastic force, the pressure forces due to the inhale,
. At each time instant, in addition to the elastic force, the pressure forces due to the inhale,  , and atmospheric pressure are acting on the valve:
, and atmospheric pressure are acting on the valve:

On the other hand:

and therefore:
 .
.
This equation is a second-order ODE with boundary-conditions  and
and  at t=0, and leads to the following solution:
at t=0, and leads to the following solution:
 .
.
Accordingly, the time it takes for the valve to reach  , equals to:
, equals to:
 .
.
The maximum closure time occurs when we assume there is no force due to pressure during inhalation,  , and it equals to:
, and it equals to:

For a silicon valve with density  2.3290
2.3290  , thickness
, thickness 
 , and radius
, and radius  , the mass of the moving section equals to
, the mass of the moving section equals to 
Assuming elasticity constant  , this formula suggests that the valve closes after
, this formula suggests that the valve closes after  .
.
Using the inspiratory flow rate time curve (pneumotachograph) of human [Fleisch 1925], the inspiratory flow rate of human at 24 ms after initializing inspiration is about 72mL/sec, and the air volume inspired in the first 24ms of inspiration is about 0.9mL. Assuming a respiratory rate of 15/min, the theoretical prediction of maximum chin valve leakage rate is about 13.5mL/min. Interestingly, this dynamic, transitory maximum leak rate is roughly the same order of magnitude as the static-pressure experimental leak-rates measured in the previous section at around NIOSH-standard suction-pressures of 25mmH2O.
Carbon Dioxide level test
The accumulation of carbon dioxide in the deadspace is a valid concern that can result in significant risks to healthcare workers utilizing respirators [18]. The accumulation of CO2 can vary greatly in snorkel masks as the connections between the inhalation and exhalation arms, the design of one-way valves, and possibly attached cartridges are very versatile. Also, the issue of CO2 buildup is not unique to full face mask snorkels nor to elastomeric respirators, but is a known factor in the continuous use of disposable N95 respirators as well [19]. For example, Lim et al., 2006 found that up to ⅓ of healthcare workers in the SARS outbreak reported headaches during use of N95 (presumably from hypercapnia) and that 4 hours of continuous use of N95 is associated with headaches [18].
To test this aspect, we utilized the mask-adapter-filter setup attached to a headform and simulated lung (Figure 12) [20, 21]. Carbon dioxide is added to the test lung at rates ranging from 200-500 mL/minute to simulate a range of metabolic output. The test lung was ventilated at respiratory rates of 12-28 breaths/minute, and tidal volumes of 400-600 mL. Gas sampling is performed with a Datex-Ohmeda gas bench at the mouth of the headform after the carbon dioxide concentration in the snorkel mask reaches steady state for at least 4 minutes. The 3 anesthesia circuit filters we tested are Teleflex Main Flow Bacterial/Viral Filter 1605, ISO-GARD Filters & Filter HMEs 28012, and Romsons HME Disposable Bacterial/Viral Filter GS-2095.
In the CO2 accumulation result, for the 3 anesthesia circuit filters we tested, the steady state CO2 concentration inside the mask is about 1~2%, which is generally safe for short term usage [20] and comparable to commercial elastomeric respirators [22]. These preliminary results are comparable to our user feedback from University of Utah, where one of our authors self-tested and reported that the work of breathing appears similar to an N95 respirator when either filter is attached. Subjectively, it appeared comfortable but took a small adjustment period to adapt to breathing to a comfortable level. At this time, we would recommend a periodic (every 5-10 minutes) deep forced exhalation to purge the mask of any CO2 buildup, which is quite similar to previously proposed solution for elastomeric respirators [19].

Figure 12: Carbon dioxide washout testing utilizing a headform and simulated lung. Various conditions are being tested to determine the suitability and safety of the proposed snorkel PPE solution in the context of carbon dioxide build up. The snorkel mask used in this setting is Dolfino Frontier.
As the risk of CO2 accumulation is directly related to the volume of dead-space, we performed direct volume measurement on our Pneumask-G setting with a Body Glove snorkel mask. The effective dead-space volume of the adapter is 10 mL while the effective dead-space volume of a Virex N100 In-line Filter is 11 mL, adding to a total volume of 21 mL, which is very low compared to the effective dead-space volume of the supplied snorkel (157mL, isolating inhalation/exhalation pathways). These results suggested that if a snorkel manufacturer has passed a CO2 accumulation test with their mask and snorkel tube, it is very likely that a Pneumaks-G based on their snorkel mask will also pass a CO2 accumulation test.
Under the same logic, it was proposed that ventilation on relaxed or resting states may conduce to CO2 accumulation due to an insufficient quenching of the mask secondary to the low minute ventilation expected during resting states. To determine if there is a difference between resting and exercise in terms of CO2 accumulation and re-breathing, a volunteer member of the team performed a “resting test”.
A male, 38 years old healthy volunteer, under standard monitoring including ECG, SatO2, NIBP, EtCO2 and Inspired CO2 measurements, wore the Pneumask in the G configuration for a total of 80 minutes. During the test, the subject lied recumbent and without moving. An anesthesiologist was present at all times during the test, recording the vital signs trend and was instructed to stop the test if vital signs deteriorated in any way. The subject could not see the monitor values to prevent from altering the normal breathing pattern in reaction to CO2 or other variable values.
The results are displayed in the following spreadsheet.
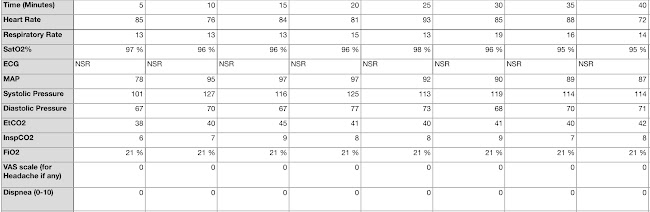
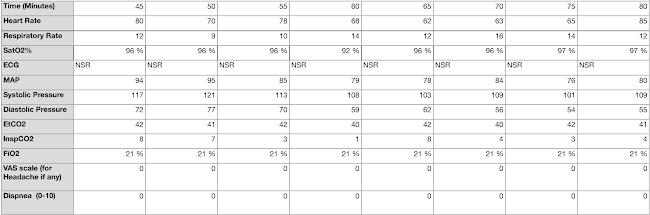
Although the was an increase in the Inspired CO2, consistent with rebreathing and insufficient quenching of exhaled CO2, with a maximum value of 9 mmHg of inspired CO2 at the minute 15 of the test, the EtCO2 values remained stable, as did all the other vital signs values for the entirety of the test. Our explanation is that the inspired CO2 rise triggered an increase in minute ventilation and respiratory rate, maintaining EtCO2 within normal values.
In conclusion, after 80 minutes of mask use under resting conditions, there was no significant accumulation of CO2 and no deleterious effects secondary to the observed elevation of inspired CO2. It is likely that any accumulation under resting conditions will be minimal and automatically adjusted by the user by the normal physiologic response to CO2 buildup.
Exercise test
Currently, 3 exercise tests have been conducted by volunteers using the Pneumask-G configuration. In the first 2 tests, the volunteer was a 38 years old male, ASA 1 status, with weight of 83kg for a height of 1.80 m (2.03 m2 total body surface area by Mosteller formula). Both tests were performed at FiO2 of 21% (ambient inspired oxygen fraction at a barometric pressure of 1011 hPa).
In the first test, a Decathlon EasyBreath mask was used with a 1.6 cmH2O pressure drop, bacterial/viral filter with no HME (Heat and Moisture exchanger). The mask has been worn on a treadmill at maximum inclination, for 10 minutes, to measure the CO2 level during intense activity. For a constant running speed of 6mph, the inhaled CO2 remained below 2mmHg at all times, while the exhaled CO2 rises up to 48mmHg on peak physical effort.
The second test was performed by the same volunteer subject, in the same treadmill machine, under same general conditions for 1 hour, with the Pneumask-G configuration but with a HMEF filter with a pressure drop of 4.5 cmH2O, which is almost 3 times higher than the filter used for the first test. For the second test, we monitored heart rate, SpO2, non-invasive blood pressure (NIBP), ECG, End-tidal CO2, Inspiratory CO2, FiO2, as well as a number of subjective measures including discomfort and stamina. The results of this test are summarized in Table 4. These results indicate that the change in Inspiratory CO2 throughout use of the device, in exertion that simulates that of most healthcare work, is negligible and in line with NIOSH standards [19]. Subjective comfort/discomfort was rated from 1 of complete discomfort to 10 of complete comfort. It is notable that this never fell below a rating of a 7. Further, the volunteer had an appropriate HR response for the level of exertion and no further alterations in physiological processes were noted. This indicates the device performs similar to elastomeric respirators under near identical conditions.
Table 4. Results of the 1 Hour treadmill test. | ||||||||||||
Time (Minutes) | 5 | 10 | 15 | 20 | 25 | 30 | 35 | 40 | 45 | 50 | 55 | 60 |
Heart Rate (min-1) | 109 | 100 | 120 | 133 | 128 | 131 | 122 | 135 | 135 | 134 | 133 | 140 |
SatO2 (%) | 99 | 98 | 98 | 97 | 97 | 96 | 97 | 96 | 97 | 97 | 97 | 97 |
NIBP S (mmHg) | 135 | 130 | 124 | 117 | 113 | 112 | 115 | 114 | 112 | 111 | 112 | 94 |
NIBP D (mmHg) | 79 | 87 | 94 | 70 | 63 | 72 | 59 | 74 | 69 | 71 | 68 | 72 |
ECG | NSR | NSR | NSR | NSR | NSR | NSR | NSR | NSR | NSR | NSR | NSR | NSR |
EtCO2 (mmHg) | 41 | 38 | 43 | 47 | 45 | 45 | 43 | 43 | 41 | 40 | 45 | 42 |
InspCO2 (mmHg) | 4 | 3 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 3 | 2 |
FiO2 | 21% | 21% | 21% | 21% | 21% | 21% | 21% | 21% | 21% | 21% | 21% | 21% |
*Subjective comfort/discomfort | 9 | 9 | 9 | 8 | 8 | 7 | 7 | 7 | 6 | 6 | 6 | 6 |
**Subjective Stamina | 10 | 10 | 9 | 9 | 8 | 7 | 7 | 7 | 6 | 6 | 6 | 6 |
Speed KPH | 3 | 5 | 5 | 5 | 6 | 5 | 5 | 5 | 5 | 5 | 5 | 5 |
Inclination (º) | 5 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 |
Room Temperature | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
Room Humidity | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
Time (Minutes) | 5 | 10 | 15 | 20 | 25 | 30 | 35 | 40 | 45 | 50 | 55 | 60 |
Fogging (0-10) | 0 | 0 | 0 | 0 | 1 | 2 | 2 | 2 | 3 | 3 | 3 | 3 |
The third qualitative testing was performed with Pneumask-G configuration on a Body Glove™ snorkel mask on one of our co-authors. A series of capnographic measurements were performed using a closed anesthesia circuit including EtCO2, pressure, volume, and flow measurements. Under normal respiration with an open mask purge valve, the EtCO2 is around 30 mmHg. Under regular simulated Operating Room activities, there was no rise in EtCO2 noted for 30 minutes. Once we closed the purge valve with tape, the EtCO2 rose to 33 mmHg with normal respiratory pattern. No rise was noted in EtCO2 with 30 minutes of regular OR activities. Work of breathing was noted to be more difficult in this setup.
Chin-Valve Closure
With regards to the Pneumask-G configuration, we have also received incoming questions from clinicians with regards to either partially blocking (using a surgical mask over the chin valve) or fully blocking the chin valve (either by epoxy or a custom “cap”) to both reduce transmission to and from the clinicians. In response, we have conducted additional CO2 test with the chin valve closed to assess the safety of this implementation.
The test was done with the Decathlon (Subea) snorkel mask with its chin valve blocked by a 3D printer adapter blocked by a rubber membrane that made an airtight seal (Fit test was performed before the test as usual upon donning, and the chin port proved to be completely sealed). CO2 sampling line was placed on the mouth chamber, in the same way as in the exercise and resting tests. The user wore the modified mask for 25-30 minutes while sitting and normally breathing and talking to a second person (simulating normal talking during a surgical procedure). The test lasted 25 minutes and was terminated upon meeting 2 main criteria first observing stable CO2 measurements over time and second, occlusion of the CO2 sampling line by water droplets. The overall outcome, the inspired CO2 quickly climbed to around 16mmHg within the first 6 minutes, as initially expected. This outcome is similar to the outcome of our CO2 test while at rest, since the washing out of exhaled air that happens under relaxed/resting conditions is slower due to shallower ventilation. As noted in that previous test, the user would usually adapt and change his ventilation pattern (deeper ventilation) automatically to quickly reduce the CO2 build-up, which kept EtCO2 within normal range during the whole test (peak values reached 40 mmHg of EtCO2). Upon a single deep ventilation CO2 significantly dropped (to values around 2 to 3 mmHg), showing effective washing of exhaled air from the mask upon increasing tidal volumes and minute ventilation. All other vital signs remained within normal physiological range.
In addition to the numerical results, the user had also experienced a minor headache or discomfort, attributed to CO2, similar to what is described with prolonged N95 respirators and similar, fogging within the eye chamber (thus reducing visibility) that increased upon exhalation and decreased with inhalation in a cyclic fashion, and increased moisture and condensation within the mouth chamber that ultimately caused the occlusion of the sampling line and termination of the test. As a conclusion, the blocking of the chin valve, although does not pose a major health risk to the user, and poses a similar breathing workload for the user compared with the Pneumask-G configuration, may not be the optimal solution. Keeping the chin valve open and placing a surgical mask over it (as it has been done extensively in real clinical scenarios) might be a better solution. Placing a second filter through an adapter on the chin port, and thus eliminating the need for the valve is also a promising option, providing several advantages such as lesser breathing workload, filtering exhaled air preventing patient/surgical field contamination, decreasing fogging improving acoustics and preventing reinhalation of CO2 even more efficiently than the open valve configuration (but adding the need for further modification of the mask, installing a second adapter and a second filter that might not be available due to stock shortage of these filters).
Simulation of CO2 Species Transport and Flow Modeling (CFD) of Pneumask
In an effort to better understand CO2 buildup with different flow path configurations in different masks, our team has also begun to build CFD models of these masks (led by Simon Ellgas, Waymo). We are in the process of building a platform to rank different designs and mask models by theoretical relative performance.
The software used was Siemen’s STAR-CCM+; the model used the segregated flow implicit unsteady solver, with the realizable k-Epsilon URANS turbulence model. Computational runtime is around 8-9 hours per exhale-inhale cycle. We are currently solving these tests using 32 cores Intel XEON on a desktop machine (not on a compute server). Mesh size is 4.8M cells, so we have 150k cells per core. The timestep is set at 0.01s, to compromise between compute speed and quality, with a CFL number around ~20.
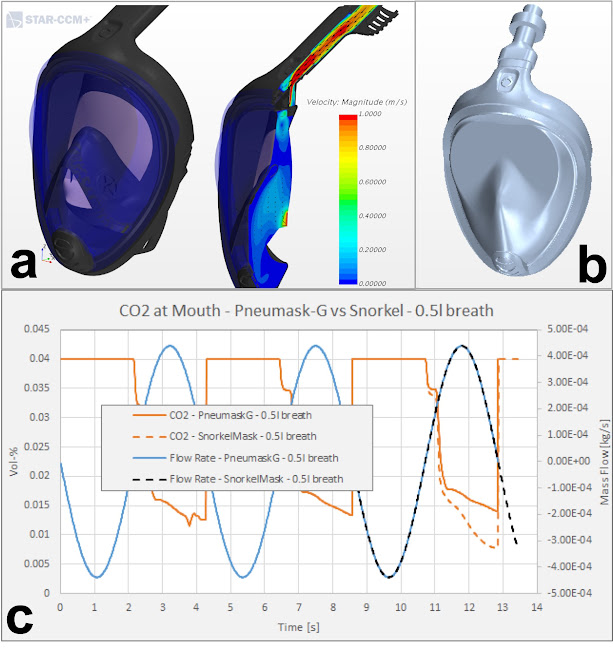
Figure 13: Preliminary results on flow modelling and species transport. a) Visualization of flow velocities within the Decathlon Easy Breath mask in stock configuration. b) Pneumask system with coupler and inline filter added. c) Preliminary CFD results on CO2 species transport, comparing the Pneumask with filter resistance to the stock configuration of the mask.
One-way valve modeling is posing some challenges numerically in the model: to avoid the numerical cost of mesh motion, and the very thin gaps present during opening and closing of the purge valves, the valves are modeled by simply varying the porous resistance of a porous region at the location of the valve. Therefore, the viscous resistance is set to a very high value to force the flow to practically zero when air would flow against the valve's direction. For flow in the valve's direction, the resistance is set to a value that reproduces the pressure drop across the valve in its full-open position. To be clear, the variable porous resistance is currently not set based on the local flow field at each valve, which would be more physical, but caused substantial numerical instability. Instead, each valve's resistance parameter is set based on the global direction of the flow (inhaling, vs exhaling). This approach is only valid since the flow changes direction almost instantaneously throughout the computational domain. While this solution is pragmatic, and allows us to perform the desired qualitative ranking of the CO2 buildup of different mask configurations with quick turn-around, it is by no means an elegant model. Furthermore, the authors are well aware of the fact that other problems of interest, e.g. potential ingress of contaminated aerosols through a valve while closing, can not be modelled with such an over-simplified approach, but would require a more elaborate representation of the one-way valves.
These computational predictions of CO2, flow rates and pressures — while they appear similar in range to experiments run at University of Utah — we caution do readers that these models were built specifically to assess relative performance of different design configurations (different flow paths, mask models, etc.) and not absolute values that could be compared to experimental tests.
We are currently extending these preliminary results to ask specific, targeted questions about relative performance of different configurations (more to follow on this thread in the coming days/weeks). Preliminary results comparing CO2 between the stock-snorkel mask and the Pneumask with filter and coupler are shown in Figure 13.
Fluid Resistance test
The fluid resistance to projectile synthetic blood of Dolfino Frontier mask and Decathlon EasyBreath v2 mask was tested following the ASTM F1862 protocol as suggested by CDC. A custom made testing box was made following the size recommendation of the protocol. After calibration of projectile speed, 2 mL of synthetic blood was projected at speed 530cm/sec and 635cm/sec to the surface lens and the chin valve of the 2 snorkel masks, and the other surface was observed for any trace of synthetic blood. The experimental setup and results are shown in Figure 14, and all testing photos are available with this link.
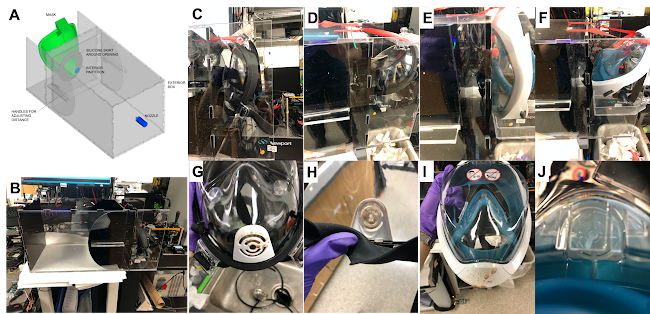
Figure 14: Fluid resistance testing on Dolfino Frontier mask (panel C, D, G, H) and Decathlon EasyBreath v2 (panel E, F, I, J). (A) The schematics and (B) the custom-made fluid resistance testing box. Both Dolfino Frontier mask and Decathlon EasyBreath masks are targeted by high speed projectile synthetic blood at the lens (C and E) and the chin valve portion (D and F). After the projection of the blood, the inner surface of the snorkel mask was checked for any contamination of synthetic blood. Both masks passed the test easily when the lens portion was targeted. When the chin valve is targeted, though synthetic blood can easily contaminate the chin valve in Dolfino Frontier mask (H), no blood is detectable from the inner surface. For Decathlon EasyBreath mask, the covering is well-designed and the entire chin valve remains clean (J).
As expected, both Dolfino Frontier mask and Decathlon EasyBreath v2 mask passed easily at both speeds when the synthetic blood was targeting the lens portion of the snorkel mask. For projectile blood targeting the chin valve, both masks also passed the test at both speeds. When the chin valve is targeted, synthetic blood can easily contaminate the chin valve in the Dolfino Frontier mask. Nevertheless, no blood was detectable from the inner surface even when the entire chin valve was contaminated. For Decathlon EasyBreath mask, the covering is well-designed and the entire chin valve remains clean even if the projectile blood was targeting the chin valve portion. These results suggested that, although both snorkel masks are safe to projectile blood, if the user is wearing a Pneumask based on a Dolfino Frontier mask, it is recommended to wash and replace the mask as soon as possible if the chin valve portion is grossly contaminated. If the user is wearing a Decathlon EasyBreath mask, it is less of a concern.
Clinical Usability Testing
The visibility of Dolfino Frontier has been extensively tested by multiple lab members, and no fogging was noted. The anesthesiologists among our co-authors also tested the same mask, and the mask did not interfere with a simulated intubation process nor with simulated standard anesthetic practices. The mask was found to reduce the volume of one's voice when worn, which can be overcome by users increasing their volume of speaking or by using our Bluetooth microphone solution. See the “Improving Communication Through Mask” section below for more information.
Improving Communication Through Mask
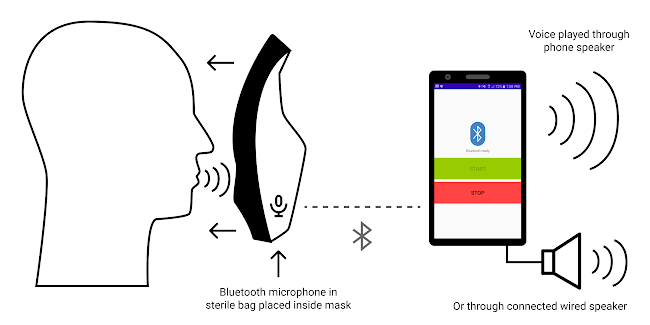
Figure 15: Diagram of Bluetooth amplification solution using only an android cell phone and wireless Bluetooth earbuds placed in the mouth part of the mask (can be placed in a plastic bag to make cleaning easier).
The full-face snorkel mask can significantly muffle the user’s voice, thereby inhibiting communication and requiring the user to strain their voice to communicate with others in a noisy environment [17]. In order to help sound travel past the mask, we created a mobile app to relay audio from a Bluetooth microphone inside the mask to speakers outside the mask (Figure 15). Sound can either be played on the phone’s internal speakers or through speakers connected to the device’s wired headphone port. The download instructions and app user instructions are available in Appendix C. All code is available on GitHub at https://github.com/kylecombes/mic-repeater-android. This solution is currently only available on Android platforms, and can be downloaded through the Google Play Store at https://play.google.com/store/apps/details?id=com.kylecombes.micrepeater. The team is currently working on some technical challenges with the iOS version, and hopes to release that soon.
Donning & Doffing Procedures
Currently we have shipped our first prototypes to Stanford and UCSF clinics, and we developed a suggested donning and doffing procedures based on the recommendation of UCSF [26] and from their preliminary feedback. A set of suggested procedures can be found in Appendix D. We will hear back with feedback soon and will share that as we proceed.
Decontamination Protocol Testing
Due to the cost and design of the full-face snorkel mask, sustainable use requires that the mask itself be reused. Thus, it will need to survive common decontamination procedures such as autoclaving or immersion in a bath of bleach or ethanol. We performed preliminary tests in which we subjected the Dolfino Frontier mask to the conditions involved in common decontamination procedures; the mask is stated by the manufacturer to consist of either silicone or thermoplastic rubber and polycarbonate lenses.
We developed and tested our decontamination protocols based on recommendations from CDC [21], OSHA decontamination protocols for respirators [7], and the consensus of National Academy of Science on reusable elastomeric respirators (p. 76) [8]. From these guidelines, a simple approach could potentially be the combined usage of detergent and bleach to achieve decontamination of the snorkel masks. Besides sodium hypochlorite, there are other hospital used disinfectants that meet EPA’s criteria for use against SARS-CoV-2 [9] or CDC guidelines on chemical disinfectant use [10]. Among these, some hydrogen peroxide solutions, such as Accelerated Hydrogen Peroxide®, offer the advantage of potentially being less harmful to the user and equipment, while only requiring a short contact time of just a few minutes. Ethylene Oxide sterilization is another commonly used method to disinfect heat sensitive equipment [11]; however, it requires specialized equipment and facilities, and whether access to such services, with the required turnaround time, is widely available to health institutions needs to be determined.
1. Autoclaving
We first performed a preliminary test to check whether mask functionality survives over the course of multiple autoclaving cycles. Before autoclaving the mask, we first took reference photos of its condition (Figure S2). We then autoclaved the mask using a 30 minute gravity cycle at 121℃ and 15 psi, with 10 minutes of warm-up before sterilization and 30 minutes of drying afterwards. Afterwards there was a mild “hot plastic smell”. Small scratches were found upon visual inspection of the black plastic material. After letting the mask rest for at least 30 minutes to cool down, we again autoclaved the mask for another identical 30 minute gravity cycle. The mask survived both cycles of autoclaving without damage. Finally, we again let the mask rest for at least 30 minutes to cool down and then autoclaved the mask for another identical 30 minute gravity cycle. After this third round of autoclaving, with a cumulative autoclaving time of 90 minutes, the silicone rubber of the mask strap and mask seal appeared to remain elastic and functional. Mask was worn after autoclaving with no apparent loss of function.
2. Bleach Immersion
Besides autoclaving, PPE may be immersed in a bath of bleach for decontamination [12]. Thus, we tested whether a mask could survive the relatively harsh chemical conditions of immersion in a bath of bleach. We immersed a new snorkel mask for 10 hours in a bath of 10% bleach. There was no apparent damage afterwards despite some white coating which can be easily washed off (Figure S3). We thus concluded that our mask should be able to survive most bleach disinfection protocols used in the hospital [7].
3. Ethanol Immersion
Besides autoclaving and immersion in bleach, PPE may be immersed in a bath of ethanol for decontamination [12]. Thus, we tested whether a new mask could survive immersion in a bath of 70% ethanol for 10 hours (Figure S4). No apparent damage was noted afterwards. (Note that we should always use 95% ethanol to make the 70% ethanol solution, since 100% ethanol may contain trace amounts of benzene which is carcinogenic.)
4. Stretch Test
With our three snorkel masks treated under three different decontamination conditions (3 cycles of autoclaving, 10 hours of bleach immersion, and 10 hours of ethanol immersion, respectively), we then performed a simple stretch test on the elastomer bands of each mask by holding the strap with both hands such that the thumbs touched each other at the tips, then pulling and qualitatively observing the separation. The straps for the ethanol-treated mask appeared to have stretched the most, while the straps for the bleach-treated mask appeared to have stretched the least. Nonetheless, all the masks are functional and seal well after all the cleaning processes.
5. Dry Heat at 65℃
Several reports indicate that dry heat at 65℃ is capable of killing any viral particles [13, 14]. Although we did not explicitly test this protocol, given the fact that the masks survived 121℃ in the autoclave for 30 minutes, we can safely infer that our mask will also survive a dry heat disinfection protocol.
6. Decontamination Summary - Guideline
Based on above testing results and the recommendation from OSHA [7], we developed suggested protocols for cleaning and decontaminating our snorkel mask (Dolfino Frontier), which is available in Appendix B. Please note that this protocol is not formally approved, and each hospital should consult their EH&S officiers or infection disease specialists for a standard operating procedure. If you are using disinfectants other than bleach, please also check this table compiled by EPA for recommended cleaning time.
Another important thing to note is that not all snorkel masks can tolerate the decontamination. For example, snorkel masks from Animdive, Tinmiu and Keystand cannot withstand the temperature of autoclave or industrial washers commonly used in OR. If you are using snorkel masks other than Dolfino Frontier, please perform appropriate testing before usage.
Failure Modes and Effects Analysis (FMEA)
We have also performed a failure modes and effects analysis on our Pneumask-G design. The analysis suggested several points that may be useful for anyone to further build upon our system: (1) using surgical hood or any additional coverage to protect the filter surface, lateral side of the mask and the straps from gross contamination (2) the pathway for inhaled air & exhaled air should be separate and pass through different filter (3) use single-usage filter if possible. For filters designed for repetitive usage, follow the instructions of manufacturers (4) avoid prolonged usage if possible (5) perform more testing on the tolerance of adapters to cleaning process (5) instructions on cleaning should specifically mention the necessity of cleaning the valve (6) development of voice amplifying system to minimize jaw movements (7) encourage face washing after doffing.
Estimated Benefit of Pneumasks during Mask Shortages
Currently there are about 953,000 practicing physicians and 3,200,000 practicing nurses in the US. According to a recent survey [3], in the US 31.4% of health care workers reported that there are no masks in their hospitals. To calculate mask requirements, we assume that each physician works 5.5 days per week and each nurses work 4 days per week, and also assume that each health care worker needs 1 N95 respirator per day. It is estimated that at least 2,578,000 N95 respirators are needed each day if every healthcare worker needs to wear an N95 respirator. If the manufacturers can provide 500,000 Pneumasks to the hospitals with severe mask shortage, it can potentially cover 62% of the current gap in mask shortage.
However, according to a recent report released by 3M [23], 3M is producing 1,167,000 N95 respirators each day, and they promised to increase production rate to 1,667,000 N95 respirators each day by June. From this discrepancy between supply and demand, we can only predict that the number of healthcare workers who have no masks to wear will continue to grow if no additional efforts are made.
As a side note, PAPR machines are unlikely to provide timely support to all the healthcare workers during this shortage. In the University of Utah Hospital, there were less than 100 PAPR machines before the pandemic, 1100 board-certified physicians and 425 beds. We can estimate the number of nurses to be 3700 based on the bed number and number of physicians. If we project the number of PAPR machines based on the machine/HCW ratio (which is more likely to be an overestimate because PAPR machines are more available in certain part of the US [24], and University of Utah Hospital is a research and teaching hospital so is likely to have more PAPR machines than average), the total number of PAPR machines available in the US is about 66,000, which is almost negligible compared to the huge demand of N95 respirators.
Elastomeric half mask respirator (EHMR) seems to be a viable alternative to N95 respirator, as one recent study shows that healthcare workers can be rapidly trained to properly wear, perform fit tests and disinfect EHMR [25]. However, the supply of this option is less clear, and it is not included in our national emergency medical equipment supply yet.
Beyond being an alternative to N95 respirators + protective goggles/face shields, Pneumasks can be combined with a disposable hood to leave no directly exposed hairs or skins that are otherwise susceptible to being contaminated with droplets (Figure 16). Without pneumasks, this kind of protection is only achievable with PAPR or the use of surgical hood/coveralls, which may also be in short supply and are associated with a more complex doffing process [27].




Figure 16: Pneumasks can be used with a disposable plastic hood to offer additional droplet protection. Also shown as references are uses of surgical hood and PAPR [27].
Regulatory Guidance
The FDA has issued Emergency Use Authorization (EUA) for PPE, including NIOSH approved respirators, which has significantly altered the clearance process for solutions such as ours. We are actively seeking guidance from the FDA for our approach in order to provide regulatory clarity to our partners and clinical sites to expedite implementation. It is our understanding that this approach will allow for NIOSH approved filtration and meet or exceed fit specifications for N95 and elastomeric respirators currently authorized by the EUA.
Upon further discussions with the FDA, we have received the following communication regarding use solutions such as the Full-Face Snorkel Mask PPE:
FDA recognizes the urgent need for face masks in the setting of the COVID-19 pandemic due to increased use and shortages in their availability.
FDA does not object to the marketing and distribution of face masks in the healthcare setting without prior 510(k) clearance if the product is labeled in the following manner:
- It states it may be used when FDA cleared masks are unavailable;
- It recommends against use in a surgical setting or where significant exposure to liquid bodily or other hazardous fluids may be expected;
- It makes no claims of antimicrobial or antiviral protection;
- It makes no claims of infection prevention or reduction;
- It makes no claims regarding flammability
- The labeling contains a list of the body contacting materials.
- The mask is not labeled as a "surgical mask”; rather it may be labeled as a “face mask”
In addition, FDA does not intend to object to marketing of masks that meet the above criteria even if they are manufactured at facilities that do not meet 21 CFR 820.
As an update, on 3/25/2020, the US FDA issued updated guidance titled “Enforcement Policy for Face Masks and Respirators During the Coronavirus Disease (COVID-19) Public Health Emergency”(FDA-2020-D-1138). In summary, this guidance now covers solutions such as the Reusable Full-Face Snorkel Mask PPE project with the following (pg3):
FDA recognizes that, when alternatives, such as FDA-cleared masks or respirators, are unavailable, individuals, including healthcare professionals, might improvise PPE. FDA does not intend to object to individuals’ distribution and use of improvised PPE when no alternatives, such as FDA-cleared masks or respirators, are available.
The CDC has published guidelines on Crisis/Alternate Strategies for PPE decisions in the setting of N95 respirator shortages. At this time, our solution can be considered a case of “HCP use of non-NIOSH approved masks or homemade masks” which is permissible in a setting where N95 respirators are so limited that routine use of them is no longer possible and surgical masks are not available. While we believe and have documented that our solution can provide higher levels of protection than homemade or simple cloth masks, we cannot make legal claims at this time until further guidance is received from regulatory authorities.
On a hospital/health system level, the University of Utah and Stanford University are actively evaluating this solution with University staff in Supply Chain, Purchasing, Value Analysis, and Infection Control as well as relevant clinical leaders. More information will be posted as this process progresses. Stanford University EH&S is also conducting independent testing as noted above.
Request for Comments
Ways to Help Out
Here is a list of the resources and help we need, for folks who would be serious about supporting and helping with our efforts:
- Feedback: If you are a doctor accustomed to local practices of your hospital in decontamination and would like to suggest a test for us to perform on these masks, please contact Hazel Soto-Montoya <hazelsoto@stanford.edu>.
- Replication: If you have access to equipment and/or supplies for decontamination protocols and would like to repeat our tests with your own equipment to check our results, please perform your own tests and let us know about your results by contacting Anesta Kothari at <anestak@stanford.edu>
- Describe the mask diversity: If you have a full-face mask that isn’t a Dolfino Frontier and some skills in the art of taking reliable measurements, feel free to make a drawing of the interface on which the tuba will connect and send it to Thibaut Pollina at <tpollina@stanford.edu> along with mask pictures or packaging for identification. If you are a supplier of these masks or know large scale distributors - please send an email to Thibaut Pollina <tpollina@stanford.edu>.
- Suggest CAD of essential adapters: You can also participate by diffusing your own CAD in step format on GrabCAD with the tag ‘COVID’. There is a need to provide an open access to all types of adapters for different full face masks (EasyBreath, Dolfino, etc) and separately for the different cartridges (3M, RD40, etc).
- Collection Drive: We are asking both retailers/suppliers and the community to donate full-face snorkel masks (of any model) that are either in stock or can be quickly mass produced in the next 1-2 weeks. We’d like to equip as many healthcare providers as possible with the proposed approach.
- 3D Printing Collaboration: We would like people to print custom attachments of our proposed design using different materials and to test which materials and attachments can be autoclaved. So if you have a 3D printer at home, please print a module, treat it with several decontamination protocols and send before and after photographs to be included here. Please send this data, along with data about your printer and printing material and your contact information and how we can credit your work, to Thibaut Pollina at <tpollina@stanford.edu>.
Documentation
We are openly sharing all working design and draft documents related to COVID-19 projects in the lab before they become finalized or ready as products. So consider this document as our idea sheet, lab notebook, and more. These are working (living) documents. But it is important to note that this is a working draft design document and is not a final solution or any medically approved device. All regulatory hurdles still need to be crossed before any patients can be served with tools.
Every week on Friday we will release an update to this document, with new partners and progress. Note that released updates will have their own revision numbers (listed in the page headers), and that these updates will be listed as named versions in the Google Docs version history for this document.
Forking and Working Independently
We will continue to release our documents and designs here so that others can help us, replicate our results, work on similar ideas independently, and/or come up with better solutions to problems identified here. We hope they will also share their solutions for open access to others globally.
Similar Concepts
Since the emergence of lack of PPE and the general lack of supplies - several other efforts are also looking at modifying snorkel masks. If you have been working on the same - please let us know to be added to this list. There are many designs available online and open source; our team can only confirm fit and accuracy data on the couplers we have personally designed.
- 3M single cartridge adapter for EasyBreath from Filip Kober shared on GrabCAD
- 3M single and double cartridge adapter for EasyBreath from Alfredo Redondo shared on Thingiverse
- RD40 cartridge adapter for EasyBreath from @realcharal #giletsjaunes shared on Thingiverse
- ISO5653 filter adapter for EasyBreath from COVID_LIFESAVER_MASK shared on Thingiverse
Map showing where our collaborators are, and some of our collaborators in action!

References
[1] Huh, S. (2020). How to train the health personnel for protecting themselves from novel coronavirus (COVID-19) infection during their patient or suspected case care. Journal of Educational Evaluation for Health Professions, 17, 10.
[2] Ranney, M. L., Griffeth, V., & Jha, A. K. (2020). Critical Supply Shortages — The Need for Ventilators and Personal Protective Equipment during the Covid-19 Pandemic. New England Journal of Medicine, NEJMp2006141.
[3] APIC. (2020). Protecting the Healthcare Workers during COVID-19 Pandemic: A Survey of Infection Preventionists.
[4] Card, K. J., Crozier, D., Dhawan, A., Dinh, M., Dolson, E., … Weaver, D. T. (2020). UV Sterilization of Personal Protective Equipment with Idle Laboratory Biosafety Cabinets During the Covid-19 Pandemic. MedRxiv, 2020.03.25.20043489.
[5] Livingston, E., Desai, A., & Berkwits, M. (2020). Sourcing Personal Protective Equipment during the COVID-19 Pandemic. JAMA - Journal of the American Medical Association. American Medical Association. https://doi.org/10.1001/jama.2020.5317
[6] 3M. (2020). Surgical N95 vs . Standard N95 – Which to Consider ?
[7]1910.134 App B-2 - Respirator Cleaning Procedures (Mandatory). | Occupational Safety and Health Administration. Available at: https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134AppB2. (Accessed: 5th April 2020)
[8] Reusable Elastomeric Respirators in Health Care. Reusable Elastomeric Respirators in Health Care (National Academies Press, 2019). doi:10.17226/25275
[9] List N: Disinfectants for Use Against SARS-CoV-2 | Pesticide Registration | US EPA. Available at: https://www.epa.gov/pesticide-registration/list-n-disinfectants-use-against-sars-cov-2. (Accessed: 5th April 2020)
[10] Chemical Disinfectants | Disinfection & Sterilization Guidelines | Guidelines Library | Infection Control | CDC. Available at: https://www.cdc.gov/infectioncontrol/guidelines/disinfection/disinfection-methods/chemical.html. (Accessed: 5th April 2020)
[11] Mendes, G. C. C., Brandão, T. R. S., & Silva, C. L. M. (2007). Ethylene oxide sterilization of medical devices: A review. American Journal of Infection Control. https://doi.org/10.1016/j.ajic.2006.10.014
[12] Lin, T. H., Chen, C. C., Huang, S. H., Kuo, C. W., Lai, C. Y., & Lin, W. Y. (2017). Filter quality of electret masks in filtering 14.6–594 nm aerosol particles: Effects of five decontamination methods. PLoS ONE, 12(10). https://doi.org/10.1371/journal.pone.0186217
[13] Darnell, M. E. R., & Taylor, D. R. (2006). Evaluation of inactivation methods for severe acute respiratory syndrome coronavirus in noncellular blood products. Transfusion, 46(10), 1770–1777. https://doi.org/10.1111/j.1537-2995.2006.00976.x
[14] Rabenau, H. F., Cinatl, J., Morgenstern, B., Bauer, G., Preiser, W., & Doerr, H. W. (2005). Stability and inactivation of SARS coronavirus. Medical Microbiology and Immunology, 194(1–2), 1–6. https://doi.org/10.1007/s00430-004-0219-0
[15] Gardner, P. D., Eshbaugh, J. P., Harpest, S. D., Richardson, A. W. & Hofacre, K. C. (2013). Viable viral efficiency of N95 and P100 respirator filters at constant and cyclic flow. J. Occup. Environ. Hyg. doi:10.1080/15459624.2013.818228
[16] McLure, H. A., Talboys, C. A., Yentis, S. M., & Azadian, B. S. (1998). Surgical face masks and downward dispersal of bacteria. Anaesthesia, 53(7), 624–626.
[17] Palmiero, A. J., Symons, D., Morgan, J. W., & Shaffer, R. E. (2016). Speech intelligibility assessment of protective facemasks and air-purifying respirators. Journal of Occupational and Environmental Hygiene, 13(12), 960–968. https://doi.org/10.1080/15459624.2016.1200723
[18] Lim, E. C. H., Seet, R. C. S., Lee, K. H., Wilder-Smith, E. P. V., Chuah, B. Y. S., & Ong, B. K. C. (2006). Headaches and the N95 face-mask amongst healthcare providers. Acta Neurologica Scandinavica, (113), 199–202.
[19] National Academies of Sciences, Engineering, and Medicine. 2019. Reusable Elastomeric Respirators in Health Care: Considerations for Routine and Surge Use. Washington, DC: The National Academies Press. https://doi.org/10.17226/25275.
[20] Caretti, D., & Coyne, K. M. (2008). Unmanned Assessment of Respirator Carbon Dioxide Levels: Comparison of Methods of Measurement. Journal of Occupational and Environmental Hygiene, 5(5), 305–312.
[21] Rutala, W. A., Weber, D. J. & HICPAC. Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008. CDC website (2013).
[22] Roberge, R. J., Coca, A., Williams, W. J., Powell, J. B., & Palmiero, A. J. (2010). Reusable elastomeric air-purifying respirators: Physiologic impact on health care workers. American Journal of Infection Control, 38(5), 381–386. https://doi.org/10.1016/j.ajic.2009.11.006
[23] Mike Roman. (2020). 3M’s collaboration on COVID-19 supply challenges and price gouging.
[24] Debra Novak (2015). Why, Where, and How PAPRs Are Being Used in Health Care. In The Use and Effectiveness of Powered Air Purifying Respirators in Health Care: Workshop Summary. National Academies Press (US).
[25] Pompeii, L. A., Kraft, C. S., Brownsword, E. A., Lane, M. A., Benavides, E., Rios, J., & Radonovich, L. J. (2020). Training and Fit Testing of Health Care Personnel for Reusable Elastomeric Half-Mask Respirators Compared With Disposable N95 Respirators. JAMA. https://doi.org/10.1001/jama.2020.4806
[26] UCSF. Droplet + contact isolation donning and doffing-sequence for putting on personal protective equipment. Available at: https://infectioncontrol.ucsfmedicalcenter.org/sites/g/files/tkssra4681/f/donning-doffing proceduredroplet-contact only.pdf. (Accessed: 5th April 2020)
[27] CDC. Ebola: Personal Protective Equipment (PPE) Donning and Doffing Procedures (for N95 and Gown). Available at: https://www.cdc.gov/vhf/ebola/hcp/ppe-training/n95Respirator_Gown/doffing_01.html (Accessed: 5th April 2020)
[28] NIOSH standard exhalation valve leakage test requirements. Specifications available at: https://www.ecfr.gov/cgi-bin/text-idx?SID=c9af10e1d89e8048667165be1f52964b&mc=true&node=pt42.1.84&rgn=div5#se42.1.84_192
Appendix A. Supplementary Tables
Table 1: List of commercially available respiratory filters which are initially designed for ventilators.
Please refer to our latest set of filters on our website: https://www.pneumask.org/filter-table
Another useful resource is the filter selection guide: https://www.pneumask.org/filter-selection-guidelines
Company | Product Names | Filtration efficiencies |
Teleflex | Main Flow Bacterial/Viral Filter (Item code 1605) | Bacterial 99.999%, viral 99.99% |
Aqua+®F Bacterial/Viral Filter (Item code 1577) | Bacterial 99.9%, viral 99.9% | |
ISO-Gard® HEPA Light with port (28002) | Bacterial and viral 99.9999+% | |
ISO-Gard® HEPA Light (28012) | Bacterial and viral 99.9999+% | |
ISO-Gard® HEPA Light Machine (28022) | Bacterial and viral 99.9999+% | |
ISO-Gard® HEPA Small, angled (28052) | Bacterial and viral 99.9999+% | |
ISO-Gard® HEPA Small, straight (28062) | Bacterial and viral 99.9999+% | |
ISO-Gard® Depth Filter (19212) | Bacterial 99.9999%, | |
Gibeck® Humid-Vent® HMEF Series (11012, 18502, 19502, 18402, 19402, 18832, 19932, 19932-BPW) | Bacterial 99.9999%, | |
GIBECK ISO-GARD (19211) - Resistance 16 mmH2O @ 60 l/min | Bacterial and viral 99.999% | |
GIBECK ISO-GARD depth filter (19212) - Resistance 20 mmH2O @ 60 l/min | Bacterial 99.999% ; viral 99.99+% | |
Philips | Bacterial Filter (Item code 342077) | Not available on website |
Bacterial Filter (Item code 1014047) | Not available on website | |
AG Industry | Not available on website | |
Medtronic | Puritan BennettTM Disposable Pediatric-Adult Expiratory Filtration System (out of stock) | Bacterial and viral 99.999%, N100 equivalent |
Puritan BennettTM Re/X800 Expiratory Bacterial Filter (out of stock) | Bacterial and viral 99.999%, N100 equivalent | |
Puritan BennettTM Neonatal Expiratory Filtration System (out of stock) | Bacterial and viral 99.99%, N100 equivalent | |
Puritan BennettTM Reusable Pediatric-Adult Expiratory Filter (out of stock) | Bacterial and viral 99.999%, N100 equivalent | |
Puritan BennettTM Re/X700 Expiratory Filter (out of stock) | Bacterial and viral 99.97%, N100 equivalent | |
Puritan BennettTM Expiratory Filter (available) | Bacterial and viral 99.97%, N100 equivalent | |
Puritan BennettTM D/X800 Expiratory Filter (out of stock) | Bacterial and viral 99.999%, N100 equivalent | |
Airon | Bacterial/Viral Filter (P/N 58210) | Not available on website |
PALL Corporation | Pall BB50T Breathing circuit filter (Item code BB50T) | Bacterial and viral 99.999% |
Ultipor® 25 Filter With Monitoring Port (Item code BB25AB) | Bacterial and viral 99.999% | |
GE Healthcare
| HMEF Neonatal bacterial viral HMEF + Luer Port | Bacterial and viral >99.9% |
Bacterial and viral 99.99% | ||
Bacterial and viral 99.999% | ||
Adult HEPA pleated paper hydrophobic bacterial viral filter + Luer port (2106570-008) | Bacterial and viral 99.99999% | |
Bacterial and viral 99.999% | ||
DAR | Bacterial and viral 99.999% | |
GVS Filter Technologies | Bacterial and viral 99.999% | |
Bacterial 99.999% - viral 99.997% | ||
Reusable Hepa Filter - Autoclavable up to 20 times | Bacterial and viral 99.999% | |
Bacterial and viral 99.999% | ||
Multi Vent Barb - Multi-ventilator filter | Bacterial and viral 99.999% | |
Bacterial and viral 99.999% | ||
Bacterial and viral 99.999% | ||
Bacterial and viral 99.999% | ||
Maxi Pleated HEPA Filter - Resistance 142 Pa | Bacterial and viral 99.9999% | |
Vyaire Medical | Hygroscopic Condenser Humidifier with Filter AirLife® Vyaire Medical 5708 | Bacterial: 99.997% |
Table 2: List of commercially available filters which are not initially designed for medical usage. More characterizations of the filtering abilities are required before using in a hospital setting. The “*” marks next to the product name indicate the ones Prakash Lab is planning to test. (N/A = not available.)
Company | Product name | Bacterial | Viral filtering | Particle size |
Cummins | Nanoforce Radial Seal Filter | N/A | N/A | 99.99% (with 0-5 um dust per ISO 5011) |
MoreWine | 99.99% | N/A | 0.45 um | |
Nispira | N/A | N/A | 99.97% for 0.3um | |
A True HEPA Filter for Germ Guard Air Purifier AC4100 Series* | 99.7% | N/A | N/A | |
A True HEPA Filter for Germ Guard Air Purifier AC5000 Series* | 99.7% | N/A | N/A | |
N/A | N/A | 0.3um, efficiency N/A | ||
99.7% | N/A | N/A | ||
Carkio | HEPA Filter Replacement Part for Bosch Gas 18V-Li 14.4v Vacuum Cleaner Accessories* | N/A | N/A | 0.3um, efficiency N/A |
Exit15 | N/A | N/A | 0.2um, efficiency N/A | |
Aerofeel | N/A | N/A | 0.4um, efficiency 60-80% | |
Dyson | N/A | N/A | 0.um, efficiency 99.97% | |
GVS Filter Technologies | EN143 + certification for infectious agents; certified for the protection against biological agents and P3 - PPE in III category. | |||
Beach | Varies based on model selected. See link for chart on filtration efficiencies by model. | |||
Table 3: List of commercially available full-face snorkel masks
Brand | Model (with link) | Size range | Price (retail) |
Cressi | S/M, M/L | 79.95 | |
Easy Snorkel | S/M, L/XL | 35.99 | |
Greatever | S, L | 36.99 | |
Guardian | S/M | 69.95 | |
Head | Sea Vision | S/M, L/XL | 64 |
Head by Mares | XS/S, S/M, L/XL | 54.99 | |
HKJB | XS, S, L | 39.98 | |
Jogoo | S/M, L/XL | 19.99 | |
Meduzi | ? | ? | |
Midry | ? | 39.97 | |
Ocean Reef | S/M, M/L | 69.95 | |
Ocean Reef | n/a | 49.95 | |
Ocean Reef | S/M, M/L, L/XL | 89.95 | |
Ocean Reef | S/M, L/XL | 60 | |
OctoberMoon | ? | ? | |
Outdoor Master (dba Greatover) | ? | ? | |
QingSong | S/M, L/XL | 35.99 | |
Seabeast | S/M, L/XL | 59.99 | |
Seac USA | Junior, XS/S, S/M, L/XL | 46 | |
Seac USA | Junior, XS/S, S/M, L/XL | 69 | |
Seac USA | Junior, XS/S, S/M, L/XL | 79 | |
Swordfish Sport | S/M, L/XL | 76 | |
Tribord (brand owned by Decathlon S.A.) | XS, S/M, M/L | 89.9 | |
Trimagic | XS, S, M, L, XL | 24.99 | |
U.S. Divers | S, M, L | 69.99 | |
Vaincre | S/M, L/XL | 24.99 | |
Wet Products | n/a | 59 | |
WildHorn Outfitters | XS, S/M & M/L | 79.99 | |
WildHorn Outfitters | S/M, L/XL | ||
X-Lounger | M, L | 27.96 |
Table 4: List of commercially available P100 respirator filters/cartridges originally for industrial usage
An explanation provided by 3M indicating the validity of using industrial use respirator filters for infection control.
Table 5.
List of EPA-certified wipes. It is ordered by required contact time. All listed products are approved for healthcare use. If a product qualifies for the emerging viral pathogen claim, it is effective against a harder-to-kill virus than human coronavirus. All products on this list meet EPA’s criteria for use against SARS-CoV-2, including those marked as “No” in this column.
Active Ingredient | Product Name | Company | Testing Viruses | Contact Time(min) | Emerging pathogen claim |
Sodium hypochlorite | Micro-kill Bleach Germicidal Bleach Wipes | Medline Industries Inc | Norovirus | 0.5 | Yes |
Hydrogen peroxide | Oxy-1 Wipes | Virox Technologies Inc | Poliovirus | 0.5 | Yes |
Quaternary ammonium; Isopropanol | Discide Ultra Disinfecting Towelettes | Palermo Healthcare LLC | Human coronavirus | 0.5 | No |
Hydrogen peroxide; Peroxyacetic acid | Peridoxrtu (Brand) One-step Germicidal Wipes | Contec Inc | Human coronavirus | 0.5 | No |
Quaternary ammonium; Ethanol | Opti-cide Max Wipes | Micro-Scientific LLC | Rotavirus | 1 | Yes |
Sodium hypochlorite | Sani-Cloth Bleach Germicidal Disposable Wipe | Professional Disposables International Inc | Adenovirus; Rotavirus; Canine parvovirus; Hepatitis A virus; Poliovirus Type 1; Rhinovirus Type 37; Feline calicivirus | 1 | Yes |
Hydrogen peroxide | Accel TB Wipes | Virox Technologies Inc | Poliovirus | 1 | Yes |
Hydrogen peroxide | Oxivir™ Wipes | Diversey Inc | Norovirus; Poliovirus Type 1; Rhinovirus Type 14 | 1 | Yes |
Hydrogen peroxide | Oxivir 1 Wipes | Diversey Inc | Enterovirus Type D68 | 1 | Yes |
Quaternary ammonium; Ethanol | Peak Disinfectant Wipes | North American Infection Control Ltd | Poliovirus Type 1; Rhinovirus | 1 | Yes |
Sodium hypochlorite | Avert Sporicidal Disinfectant Cleaner Wipes | Diversey Inc | Human coronavirus | 1 | No |
Quaternary ammonium; Isopropanol | Super Sani-Cloth Germicidal Disposable Wipe | Professional Disposables International Inc | Rhinovirus 39; Adenovirus | 2 | Yes |
Hydrogen peroxide | Clorox Commercial Solutions® Hydrogen Peroxide Cleaner Disinfectant Wipes | Clorox Professional Products Company | Norovirus | 2 | Yes |
Quaternary ammonium | Nugen 2m Disinfectant Wipes | Lonza LLC | Human coronavirus | 2 | No |
Quaternary ammonium | Caterpillar | Reckitt Benckiser | Human coronavirus | 2.5 | No |
Quarternary ammonium; Isopropanol | Opti-Cide 3® Wipes | Micro-Scientific LLC | Rotavirus; Rhinovirus | 3 | Yes |
Quaternary ammonium | AF3 Germicidal Disposable Wipe | Professional Disposables International Inc | Rotavirus; Adenovirus | 3 | Yes |
Quaternary ammonium; Ethanol; Isopropanol | Caviwipes 1 | Metrex Research | Adenovirus | 3 | Yes |
Sodium hypochlorite | Caviwipes Bleach | Metrex Research | Feline calicivirus | 3 | Yes |
Quaternary ammonium | PJW-622 | Clorox Professional Products Company | Rotavirus | 3 | Yes |
Sodium hypochlorite | Clorox Healthcare® Bleach Germicidal Wipes | Clorox Professional Products Company | Canine Parvovirus; Feline Parvovirus | 3 | Yes |
Quaternary ammonium; Ethanol; Isopropanol | Sani-Cloth Prime Germicidal Disposable Wipe | Professional Disposables International Inc | Feline Calicivirus | 3 | Yes |
Quaternary ammonium | Sani-cloth Germicidal Disposable Cloth | Professional Disposables International Inc | Human coronavirus | 3 | No |
Quaternary ammonium | Clorox Disinfecting Wipes | The Clorox Company | Rotavirus | 4 | Yes |
Quaternary ammonium | Clorox Commercial Solutions® Clorox® Disinfecting Wipes | Clorox Professional Products Company | Rotavirus | 4 | Yes |
Quaternary ammonium | Lonza Disinfectant Wipes Plus | Lonza LLC | Human coronavirus | 4 | No |
Quaternary ammonium | Nugen Low Streak Disinfectant Wipes | Lonza LLC | Human coronavirus | 4 | No |
Quaternary ammonium | Clorox Healthcare® VersaSure® Wipes | Clorox Professional Products Company | Norovirus | 5 | Yes |
Ethanol | PURELL Professional Surface Disinfectant Wipes | GOJO Industries Inc | Norovirus | 5 | Yes |
Phenolic | Sporicidin (Brand) Disinfectant Towelettes | Contec Inc | Human coronavirus | 5 | No |
Appendix B. Suggested Decontamination Protocols
Cleaning and Decontamination Protocol (Not an Approved Protocol)
- Perform hand hygiene.
- Put on a gown, gloves, and a protective mask.
- Wipe the surface of the filter with 70% ethanol or hydrogen peroxide, and carefully remove the filter.
- Discard the wipe as biohazardous waste. Discard the filter if it is intended for single-use only. If you plan to reuse the filter, follow the instructions from the manufacturer of the filter to store it properly, and DO NOT WET the surface of the filter.
- Wash mask and filter adapter thoroughly in warm water (43℃ [110℉] maximum) with a mild detergent. A sponge that won’t scratch may be used to facilitate the removal of dirt. Make sure to clean all the valves to avoid potential clogged valves.
- Rinse the mask and adapter thoroughly in clean, warm (43℃ [110℉] maximum), running water. Drain.
- Prepare a 50ppm chlorine solution: add one milliliter of laundry bleach per liter of warm water (43℃ [110℉] maximum). Prepare enough solution to fully immerse the entire mask. Remove all the air in the side channel to ensure full immersion. Please note that mixing bleach solutions with detergents can generate toxic substances. Make sure to wash out all the detergents before immersing the mask and adapter into bleach.
- Immerse the mask and adapter in the hypochlorite solution (50 ppm of chlorine) for 2 minutes.
- Wearing fresh gloves, rinse the mask and adapter thoroughly in clean, warm, running water (43℃ [110℉] maximum). The mask and adapter must be thoroughly rinsed with water to remove any detergents or disinfectants that may result in dermatitis or damage of the mask components.
- Dry the mask and adapter with a clean lint-free cloth or allow to air dry.
- Reassemble the mask and store in a clean space.
This protocol is based on OSHA's procedure for cleaning respirators:
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134AppB2
Appendix C. Communication App User Instructions
Current Android app download instructions:
- Download the beta version of the app by visiting http://kylecombes.com/app-debug.apk on your phone.
- Open the download. Your phone should prompt you to allow installations from unknown (i.e. non-Google Play) sources. If it does, simply follow the on-screen instructions. If no such prompt appears and the installation merely fails, do the following:
- Allow app installations from unknown sources by going to your phone’s Settings -> Security -> Unknown Sources and enable installations. This setting might have a different name, depending on your version of Android and device manufacturer.
- Try to install the app again by re-opening the download or revisiting the link above.
App usage instructions:
- Connect your phone to a Bluetooth device with a microphone. We recommend using cheap Bluetooth headphones, which can be put inside a sterilized plastic bag, and placed inside the face compartment of the snorkel mask.
- (Optional, for extra amplification) Connect an external speaker to the phone’s wired headphone jack using an aux cord. If you do not do this, the phone will use its internal speakers.
- Open the app.
- If the app detects a Bluetooth device capable of streaming audio, it will say “Bluetooth ready.” If it does not, follow the on-screen instructions to ensure your device is connected properly.
- Click “Start” to begin relaying audio from the microphone to the speaker.
- You may now turn off the phone’s screen or switch to another app if you would like. If you need to switch speakers at any point, click “Stop,” do any plugging/unplugging, and then click “Start.”
- Click “Stop” end relaying audio.
Troubleshooting:
If the sound is playing out of the Bluetooth speaker instead of through the wired speaker, simply unplug and replug in the wired speaker.
Currently, the iOS version of this app is under development, and the Android app is pending publication in the Google Play Store. Please reach out to the provided contacts if you have any feedback, questions, or concerns.
Contacts: Emma Pan (epan549@gmail.com), Kyle Combes (kcombes@olin.edu)
Appendix D. Suggested Donning/Doffing procedures
***further review of this protocol by infection disease specialists or EH&S officers in hospitals is required.**
Donning Procedures
- Eat, drink and go to the restroom. Check everything that you need to bring into the patient's room is available.
- Tie up your hair and remove unnecessary accessories on wrists, neck and ears.
- Perform hand hygiene.
- Put on a surgical cap, tucking loose hair away from the face and neck.
- Put on the first layer of gloves.
- Put on your gown by placing your head through the top of the opening and insert your arms into the sleeves. Tie the gown properly.
- Carefully inspect the disinfected snorkel mask, adapter and viral filter of Pneumask.
- (Optional if they are connected already) Serially connect the adapter and viral filter to the snorkel mask.
- (Optional for Bluetooth user) Turn on the Bluetooth microphone. Check the connection with the smartphone. Put the Bluetooth microphone in a clean, small ziplock bag, Tape and secure the ziplock bag inside the mouth chamber without blocking the chin valve.
- Perform a suction test: put the mask to your face, press it slightly while inhaling to create a suction between the mask and your face. The mask should suction to your face. Try smiling and see if the movement of facial muscle breaks the seal. IF MASK DOES NOT PASS SUCTION TEST, THE MASK SHOULD NOT BE USED.
- Put on the mask fully. Adjust and tighten the straps as needed.
- Inhaling or exhaling while closing off the top of the filter with your hand can be done for another seal check. With a good facial seal, the mask should suck down on your face with a good seal with inspiration, and not lift off face with exhalation.
- Perform hand hygiene.
- Place your gloved thumbs through the loops of the gown. Put on the second layer of gloves.
Doffing Procedures
- In the anteroom (or the doorway if there is no anteroom), grasp the gown and pull away from your body. Carefully fold the gown into ball-shape and only touch the outer surface of the gown with gloved hands. Remove the gown and the outer gloves together. Dispose the gown and the gloves into a dedicated trash can.
- Perform hand hygiene (you should still be wearing your inner layer of gloves).
- Leave the anteroom.
- Perform hand hygiene.
- Inspect the integrity of the inner glove.
If the inner glove is intact without gross contamination, proceed through the next step.
If the inner glove is torn, broken, or grossly contaminated, remove the inner glove. Perform hand hygiene, and put on a new pair of gloves. - Lean head forward into sniff position. Loosen the straps and remove the mask without touching your face.
- Use EPA-approved alcohol-based wipe, bleach wipe, AF3 wipe or hydrogen peroxide wipe to wipe the outer surface of the mask, adapter and filter. Dispose the wipe. The required contact time for different EPA-approved wipes can be found in Appendix A Table 5.
- Use another EPA-approved alcohol-based wipe, bleach wipe, AF3 wipe or hydrogen peroxide wipe to wipe the inner surface edges of the mask. Dispose the wipe.
- Gently disconnect the filter from the mask. Dispose the filter if it is designed for one-time usage. If you plan to reuse the filter, follow the instructions from the manufacturer of the filter to store it properly, and DO NOT WET the surface of the filter.
- Put the mask into a clean dedicated box.
- Perform hand hygiene.
- Remove the surgical cap.
- Perform hand hygiene.
- Remove the inner gloves.
- Perform hand hygiene.
- (Optional for Bluetooth user) Remove the ziplock bag which contains the Bluetooth microphone. Wipe the surface of the ziplock bag with EPA-approved wipe (Appendix A Table 5) and open the ziplock bag. Perform hand hygiene. Dump the microphone from the ziplock bag with one hand (dirty hand) onto the other hand (clean hand). Dispose the ziplock bag with your dirty hand. Place the microphone somewhere you will not forget with your clean hand. Perform hand hygiene.
- By the end of the shift, bring the box and the mask to somewhere you can fully decontaminate it following our decontamination protocol, or hand it to hospital technicians per hospital policy. The recommendation of using disinfection wipe between patients and fully washing it after one shift is following the recommendation of NIOSH on elastomeric respirator.
Appendix E. Supplementary Figures
Dolfino Frontier | Seaview 180 V1 | Easybreath V1 | Ocean Reef Aria | DIVELUX |
Tested model | To be tested | Original model | To be tested | To be tested |
Waiting for CAD | Waiting for CAD | |||
WMM17478SBK |






Figure S1: (A) Table of various full-face snorkel masks readily available in the market with links. (B) Evolution of the prototype of full-face snorkel masks over time by the original inventors - Subea Team.
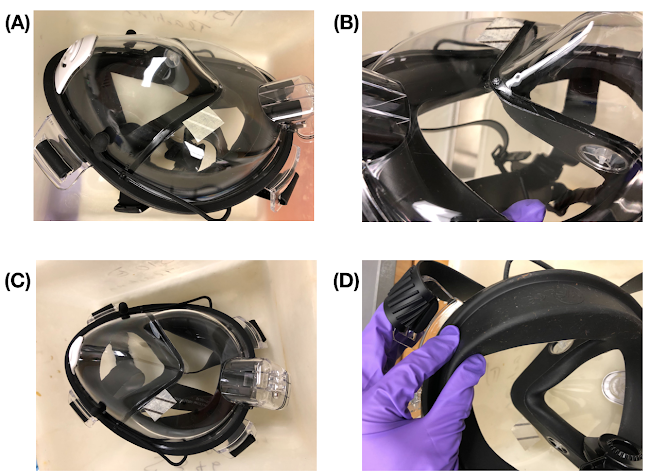
Figure S2: Before Autoclave (A), Round 1 (B), Round 2 (C) Round 3 photos and video (D). The mask survives autoclaving at 121℃ and 15psi for a total of 90 minute cycle (done in three cycles of hot and room temperature) without apparent damage. The folders of photos and/or videos are available with the link in the caption.
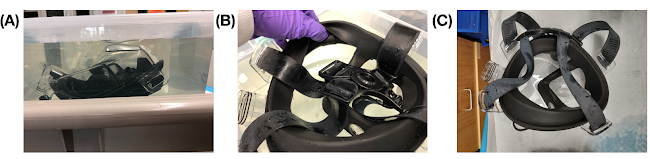
Figure S3: (A) Mask immersed in 10% bleach in a simple tupperware. (B) After 2 hours of immersion, we found no apparent damage to the mask. (C) After 8.25 additional hours of immersion, we again observed no apparent damage to the mask, though white coating had formed on the surface of the black elastomer bands.
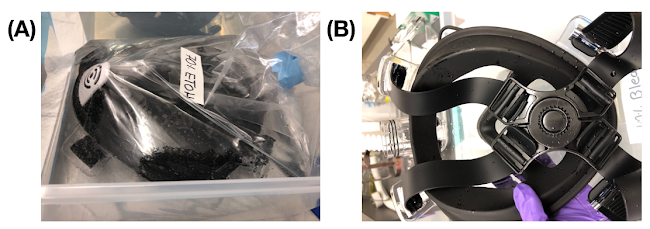
Figure S4: (A) Before (B) After 2 hours of immersion, we found no apparent functional damage to the mask.
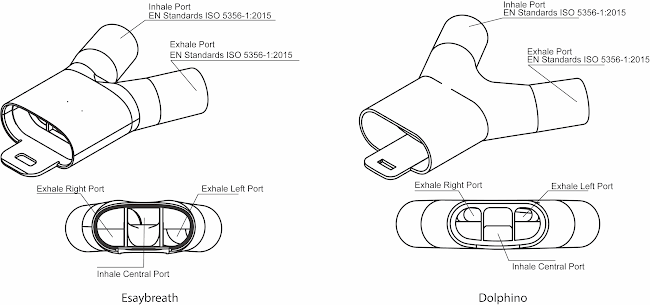
Figure S5: Dolphino and Easybreath double port inhale/exhale separation adapters. The design followed EN Standards ISO 5356-1:2015. A set of connectors ISO 5356 are available on GrabCAD thanks to Filip Kober. The CAD files of the universal adapter for Easybreath (https://a360.co/2Ukh6w5) and Dolphino Frontier (https://a360.co/39jnJCQ) are available with the links provided.
Figure S6: We have developed a nomenclature of the different combinations existing for the air flow pathway. Pneumask-G could then be named 1-f/Cvex and Pneumask-S named 2-If-Ov/Cx. Notation: diodes = one-way valves; resistor = filter. Please find the .ai original vector file here.