



Managing small pupil challenges in patients with the Malyugin ring
The Malyugin ring 2.0 expands the small pupil safely and effectively to enable excellent intraoperative visualisation. It has a good safety record and is easier to use than alternative methods.



Adequate visualisation of the lens is necessary for safe cataract surgery, and the best way to achieve this is with dilated pupils. Inadequate pupil dilation can lead to surgical complications including iris damage, bleeding, prolapse, intraoperative floppy iris syndrome (IFIS), anterior capsule trauma and misalignment of the IOL. All of these are best avoided by ensuring you have a wide pupil.
Current approaches to small pupil management include cutting the iris at its edge, stretching the pupil mechanically using two side instruments, the use of iris hooks, heavy viscoelastic application and pharmacological dilation, or pupil expansion devices such as the Malyugin ring 2.0 (MicroSurgical Technology).
This is an innovative device that was initially designed by Prof. Boris Malyugin to expand the small pupil safely and effectively as a solution to the potential overstretching of the iris sphincter or extended surgery time.1 I think the Malyugin ring is one of the best tools to dilate the pupil and maintain that dilation intraoperatively, therefore streamlining even the more challenging cataract cases.
Challenging cases
The ring is manufactured with 5.0 polypropylene, which is a thin (<1.0-mm) and flexible material. This makes it elastic, so it causes less damage to the iris compared with other devices. It also features a large scroll gap that eases the engagement of the iris and removal of the ring.
I use both sizes of the Malyugin ring, 6.25 mm and 7.0 mm, depending on the diameter of the eye and the individual pupil. Sometimes the anterior segment is small, especially in hyperopic eyes, in which case it would be difficult to insert the larger size. In myopic eyes, I tend to use the bigger size.
The size chosen will also depend on the thickness of the iris as some can be stiff, especially in post-traumatic eyes, and it can be challenging to place the eyelets precisely in the iris. So, it depends on the situation and the individual case.
There are essentially two main cases where I use the Malyugin ring 2.0 in surgery. One is when there is a small pupil with no synechiae. Small pupils with no synechiae can result from alpha-blocker treatment, IFIS or other conditions. In cases of small pupils with synechiae, it is necessary to release all adherences between the iris and the lens before placing the device.
Other cases where I use the ring often include an exchange to a posterior lens due to subluxation. In these cases, I aim to keep the pupil dilated to see precisely where the lens and the bag are in the posterior segment of the eye.
Note: IFIS can complicate cataract surgery and can frequently occur in patients taking alpha-blocker medications such as tamsulosin (Flomax, Astellas). Physicians often prescribe alpha-blockers for the treatment of benign prostatic hyperplasia, to women with urological issues and patients with hypertension.
Insertion and removal
At first, I use a pharmacological product such as adrenaline to dilate the pupil. If working under topical anaesthetic, I advise adding non-preserved 1% lidocaine, resulting in intracameral anaesthesia, and adding modest dilation by paralysing the nerves in the iris. Currently, my preference for pharmacological dilation is Mydrane (tropicamide 0.2 mg/mL, phenylephrine chlorhydrate 3.1 mg/mL, lidocaine chlorhydrate 10 mg/mL; Thea).
Synechiae need to be released before inserting the Malyugin ring. First, one should break the posterior synechiae with a cyclodialysis spatula or cannula. I like to use a blunt cannula; for instance, a LASIK cannula. Ensuring all the synechiae are released is of paramount importance as I do not want any remaining under the iris.
Mechanical dilation follows. In this step, I will simply stretch the small pupil using a Lester hook and capsulorhexis forceps. This bi-manual technique allows me to dilate linearly and then at a 90-degree angle.
Before inserting the ring, I add more viscoelastic device into the eye to lift the iris from the anterior capsule. The device comes with an injector for easy insertion and removal and is specifically designed to be implanted through a 2.0-mm incision.
My approach to insertion
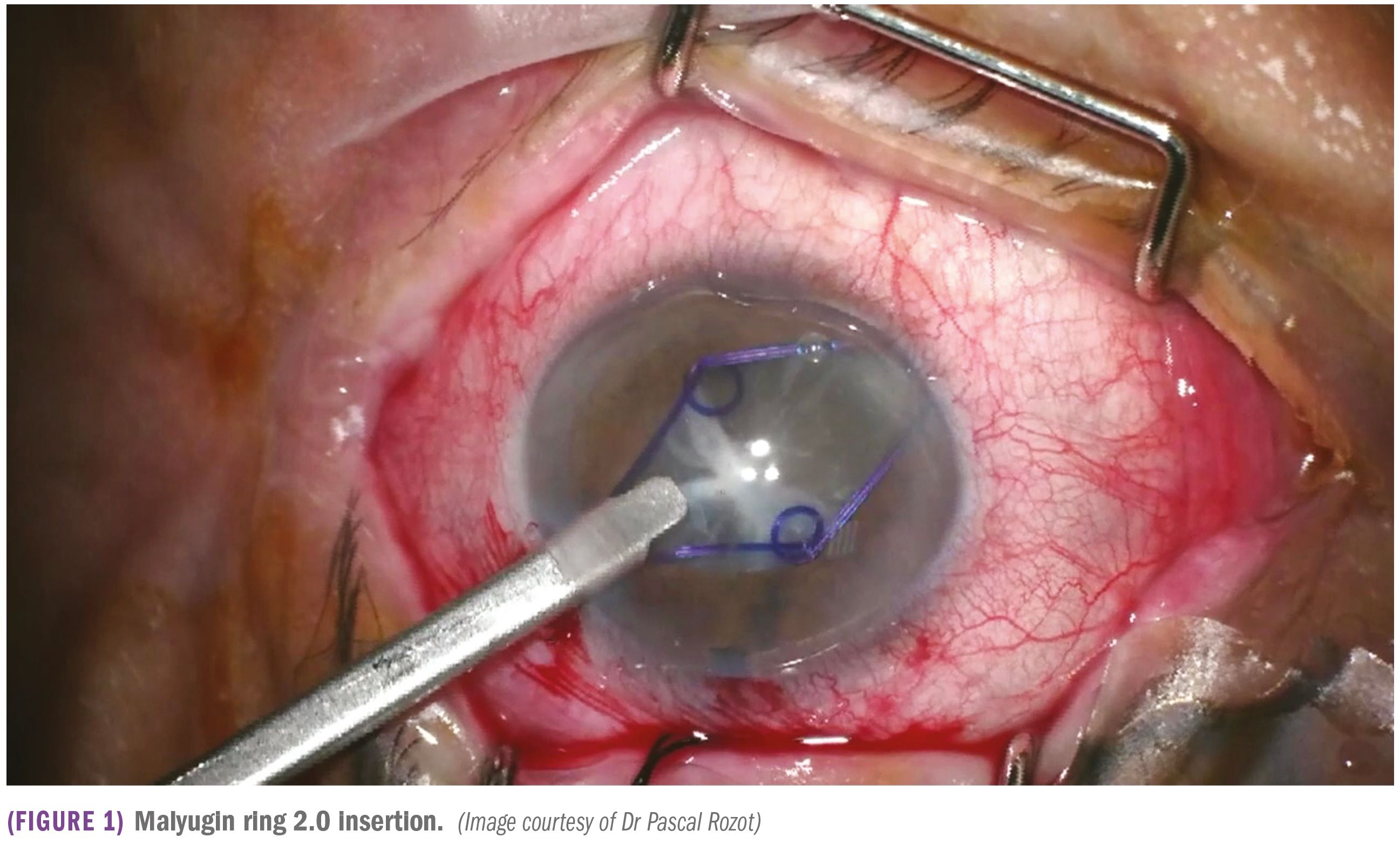
I normally insert the Malyugin ring injector upside down through the incision with the footplate on top. This allows me to get closer to the iris with the injector to engage the first three scrolls of the ring as it is released from the injector (Figure 1).


To remove the ring, I disengage the scrolls to lift it above the iris plane. Again, I use the injector upside down; I grasp the proximal scroll with the injector hook and the ring is retracted using a sliding mechanism. Insertion of the ring requires the skill of the surgeon, a skill that comes with experience using the device.
Conclusion
The Malyugin ring 2.0 is, for me, the pupil expander of choice: it exhibits precision, is easier to use than iris hooks,2 has a good safety record and allows excellent intraoperative visualisation. It essentially changes complicated cataract surgery into a routine procedure.
---
Pascal Rozot, MD
E: pascal.rozot@dr-rozot.com
Dr Rozot is an ophthalmic surgeon based in Marseille, France. He specialises in refractive cataract surgery, management of complex cataract cases, such as post-traumatic or congenital, and surgical treatment of glaucoma. He has no financial interest in the subject of the article.
References
- Malyugin B. MicroSurgical Technology: The new generation of the Malyugin Ring 2.0. Available at: https://www.youtube.com/watch?v=8_5qWnBDxNg.
- Nderitu P, Ursell P. Iris hooks versus a pupil expansion ring: Operating times, complications, and visual acuity outcomes in small pupil cases. J Cataract Refract Surg. 2019;45:167–173.

















